Epidemiology of HPV Cancers
-
1) How Prevalent Are Genital HPV infections In The US?
 A review published in 2024 looked at social determinants of health and how they effect the stage of when oropharyngeal cancers (those caused by HPV as well as those that are not) are diagnosed. Being black, male, lacking insurance, rurality, and low socioeconomic status were all identified as risk factors for advanced stage at presentation.
A review published in 2024 looked at social determinants of health and how they effect the stage of when oropharyngeal cancers (those caused by HPV as well as those that are not) are diagnosed. Being black, male, lacking insurance, rurality, and low socioeconomic status were all identified as risk factors for advanced stage at presentation.
Ioerger, P. et al Inequities Associated With Advanced Stage at Presentation of Head and Neck Cancer: A Systematic Review. JAMA Otolaryngol Head Neck Surg. doi:10.1001/jamaoto.2024.1180
According to the CDC:
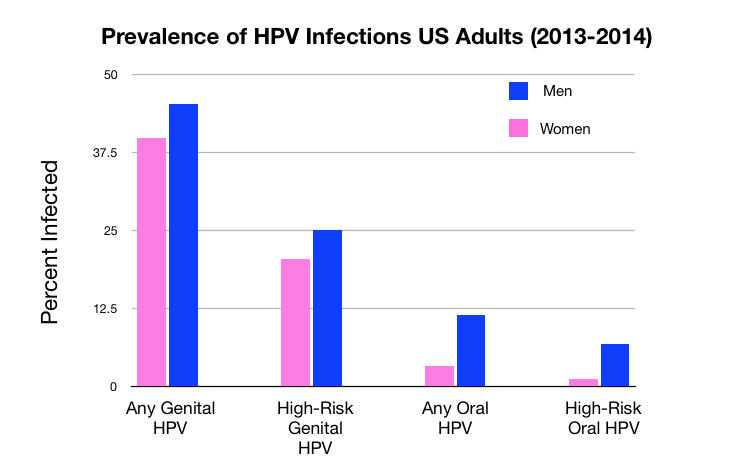
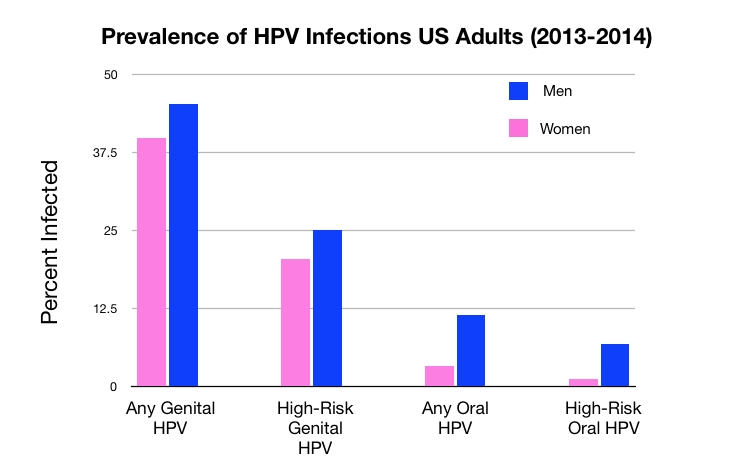
During 2013–2014, prevalence of any genital HPV was 42.5% among adults aged 18–59, 45.2% among men and 39.9% among women.
Overall, and for both men and women, prevalence of any genital HPV was lowest among non-Hispanic Asian adults and highest among non-Hispanic black adults, with no significant difference in prevalence between non-Hispanic white and Hispanic adults.
Prevalence of any genital HPV was higher among men than women overall and among non-Hispanic white adults. The pattern was similar for Hispanic adults, but the difference between men and women was not statistically significant.
Prevalence of high-risk genital HPV was lowest among non-Hispanic Asian adults and highest among non-Hispanic black adults.
During 2013–2014, the prevalence of high-risk HPV was 22.7% among adults aged 18–59, 25.1% among men and 20.4% among women.
Overall, and for both men and women, prevalence of high-risk genital HPV was lowest among non-Hispanic Asian adults and highest among non-Hispanic black adults, with no significant difference in prevalence between non-Hispanic white and Hispanic adults.
Prevalence of any genital HPV was higher among men than women overall and among non-Hispanic white and non-Hispanic black adults.”
A more detailed look at racial disparities in occurrence of HPV-caused cancers and how the availability of the vaccine has not alleviated this can be found in: Burger et al Racial and ethnic disparities in human papillomavirus (HPV)- associated cancer burden with first- and second-generation HPV vaccines. Cancer. 2016 July 1; 122(13): 2057–2066. doi:10.1002/cncr.30007.
—————————————————————————————————————————————————
In a separate study, the prevalence of any genital HPV strain was measured in women and the results were tabulated according to their age. The study was conducted as part of the National Health and Nutrition Examination Survey (NHANES) in 2003-2004, before the introduction of the HPV vaccine in the US. You can read the demographic info in the paper itself. Women were between the ages of 14 and 59.
Overall findings:
Age Range Percent Positive for HPV
14-19 25%
20-24 45%
25-29 27%
30-39 28%
40-49 25%
50-59 20%
Details: Dunne, E.F. Prevalence of HPV Infection Among Females in the United States. JAMA. 2007;297(8):813-819. doi:10.1001/jama.297.8.813 FREE Download
About 40% of pregnant women in the US have an HPV infection, and HPV could be detected in 10% of placentas. Only 7% of neonates had HPV at birth, and no infection persisted at 6 months.
Khayargoli, P.et al JAMA Pediatr. Published online May 22, 2023. doi:10.1001/jamapediatrics.2023.1283-
2) How Prevalent Are Oral HPV Infections In The US?
 According to the CDC:
According to the CDC:
“During 2011–2014, prevalence of any oral HPV was 7.3% among adults aged 18–69, 11.5% among men and 3.3% among women
Prevalence of any oral HPV was lower among non-Hispanic Asian adults (2.9%) and higher among non-Hispanic black adults (9.7%) compared with both non-Hispanic white (7.3%) and Hispanic adults (7.0%). For men, there was a similar racial and ethnic pattern.
Prevalence of any oral HPV was lowest among non-Hispanic Asian women. No significant difference in prevalence was seen among non-Hispanic white, non-Hispanic black, and Hispanic women.
Men had a higher prevalence of oral HPV than women, overall and within each race and Hispanic group.
Prevalence of high-risk oral HPV was lower among non-Hispanic Asian adults compared with other race and Hispanic groups:
During 2011–2014, prevalence of high-risk oral HPV was 4.0% among adults aged 18–69, 6.8% among men and 1.2% among women.
Prevalence was lower among non-Hispanic Asian adults, overall (1.7%) and among men (2.3%), than non-Hispanic white (4.2% all, 7.3% men), non-Hispanic black (4.3% all, 7.5% men), and Hispanic (3.4% all, 5.4% men) adults.
No differences were seen in prevalence of high-risk oral HPV by race and Hispanic group among women (1.1%–1.7%).
Prevalence of high-risk oral HPV was higher among men than women in all race and Hispanic groups, although the difference was not significant among non-Hispanic Asian adults.”
In terms of survival of HPV-caused oropharyngeal cancers, whites, hispanics, and asians have very similar rates, but blacks have a much worse survival pattern.
Faraji, F. et al The Prevalence of Human Papillomavirus in Oropharyngeal Cancer Is Increasing Regardless of Sex or Race, and the Influence of Sex and Race on Survival is Modified by Human Papillomavirus Tumor Status. Cancer 2018. DOI: 10.1002/cncr.31841
Here’s a different look at similar data focused just on HPV driven oropharyngeal cancer, in this case broken down by ethnic/racial groups and by gender. Note that men have higher rates of this cancer than women at every age, and in every ethnic group. Source: Mahal, B.A. et al Incidence and Demographic Burden of HPV-associated Oropharyngeal Head and Neck Cancers in the United States. Cancer Epidemiol Biomarkers Prev Published OnlineFirst July 29, 2019
Overall, about 47% of all head and neck cancers are caused by HPV (2016 data). These are broken down by anatomical location in the chart below. The 47% figure was derived by adding up the total number of cases of HPV cancers at all anatomical locations (20,958) and then dividing that by the total number of head and neck cancers (44,419). Source: Ellington, T.D. et al Trends in Incidence of Cancers of the Oral Cavity and Pharynx — United States 2007–2016. CDC MMWR Weekly / April 17, 2020 / 69(15);433–438. FREE download
See FAQ 30 below for details about racial disparities with oral HPV-cancer survival.As indicated above, the oral cavity is not a site where HPV cancers are generally found. The prognostic impact of HPV in oropharyngeal cancer is generally acknowledged, and HPV‐status is assessed routinely in clinical practice. Paradoxically, while the oral cavity seems the predilection site for productive HPV‐infections, figures on HPV‐attribution in oral cavity squamous cell carcinoma (OCSCC) differ widely, and prognostic impact is uncertain. A recent study looked at all OCSCC‐patients diagnosed between 2008‐2014 at two Dutch university medical centers (N=1,069). In total only 21 (2.2%) OCSCCs were HPV DNA‐positive. All HPV DNA‐positive tumors were E6 mRNA‐positive and considered as true HPV‐positive. There was no difference in survival between HPV‐positive and HPV‐negative OCSCCs. Survival was similar in p16‐positive and p16‐negative OCSCCs. Conclusion: HPV‐prevalence is very low in OCSCC, and neither HPV‐status nor p16‐status affects outcome. Based on these data, determining HPV‐status in OCSCC seems irrelevant.
Naruta, I.H. et al The unveiled reality of human papillomavirus as risk factor for oral cavity squamous cell carcinoma. https://doi.org/10.1002/ijc.33514-
3) Is The Incidence Of Oral Cancers Soaring In Men?
Hokusai’s The Great Wave (Re-interpreted by Josh and Stewart Lyman)
This is true. In the US, the number of yearly cases of HPV-caused oropharyngeal tumors has more than doubled between 1999 and 2015. It went from 6,996 cases in 1999 to 15,479 cases in 2015 (an increase of 121 percent).
HPV prevalence of oropharyngeal cancers increased from 16.3% during 1984 to 1989 to 71.7% during 2000 to 2004. This reflects both the spread of HPV as well as a decline in HPV- negative oropharyngeal cancers caused by smoking and drinking.
According to the CDC, in 2015, oropharyngeal cancers made up 82% of all HPV-cancers in men, followed by anal cancers (12%) and penile cancers (6%).
The percentage of oropharyngeal cancers that were HPV positive increased from 16.3% in the period 1984–1989 to over 70% in 2000–2004 in the United States. This increase is highest among middle-aged white men (40 to 59 years old). Reference: Pytynia KB et al Epidemiology of HPV-associated oropharyngeal cancer Oral Oncol. 2014 May ; 50(5): 380–386. doi:10.1016/j.oraloncology.2013.12.019.
In oropharyngeal cancers, HPV 16 is the most common high-risk infection. HPV 16 accounts for 90% of HPV-related OPCs. Reference: Guo T et al The Potential Impact of Prophylactic HPV Vaccination on Oropharynx Cancer. Cancer. 2016 August 1; 122(15): 2313–2323. doi:10.1002/cncr.29992.
This increasing frequency of HPV-caused oropharyngeal cancer is also increasing in women! While many more men than women develop HPV-caused oropharyngeal cancers (OPC), the rate is actually INCREASING in both men AND women. In 2010 the prevalence of HPV-caused OPC was 64.9% in men and 54.1% in women, by 2015 its prevalence had grown to 75.2% in men and 60.5% in women. Interestingly, the prevalence of HPV positivity increased by 3.5% per year for men and 3.2% per year for women.
Men and women have pretty similar survival curves following diagnosis with HPV+ oropharyngeal cancers. Five year survival rates are close to 80%, with longer survival associated with less extensive disease at diagnosis. Nearly twice as many patients with HPV negative oropharyngeal cancer present with lymph node involvement compared to patients with HPV positive oropharyngeal cancer.
The ratio of HPV+ to HPV- oropharyngeal cancers in men is about 2.4 to 1; in women it’s only about 1.3 to 1.
Faraji, F. et al The Prevalence of Human Papillomavirus in Oropharyngeal Cancer Is Increasing Regardless of Sex or Race, and the Influence of Sex and Race on Survival is Modified by Human Papillomavirus Tumor Status. Cancer 2018. DOI: 10.1002/cncr.31841
This topic has been widely covered in the popular press: e.g. Oral HPV More Common in Men Than Women NY Times 2012
Here are 5 recent papers focused on this issue:
HPV Related Disease Burden and Impact of HPV Vaccine (2018) by Martin Mahoney, MD, PhD Roswell Park Cancer Institute
Oropharyngeal Cancer Epidemiology by Kristina R. Dahlstrom, Ph.D. MD Anderson Cancer Center
Oropharyngeal Cancer: Clinical Implications of the HPV Epidemic by Erich M. Sturgis, M.D., M.P.H.
Epidemiological Trends of Head and Neck Cancer in the United States: A SEER Population Study Mourad et al J Oral Maxillofac Surg 75:2562-2572, 2017
Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States Chaturvedi et al J Clin Oncol. 2011 Nov 10; 29(32): 4294–4301
Prevalence of Oral HPV Infection in the United States, 2009-2010 by Gillison et al JAMA. 2012;307(7):693-703
This is not only happening in the US. Here’s a report of a similar phenomenon in Sweden:
Incidence of human papillomavirus (HPV) positive tonsillar carcinoma in Stockholm, Sweden: An epidemic of viral‐induced carcinoma?
—————————————————————————————————————————————————————————————————————
In an international study, oral gargle samples from 3,095 men in the multinational HPV Infection in Men (HIM) Study were HPV genotyped. Multivariable models assessed factors independently associated with high-risk and low-risk HPV prevalence. The prevalence of high-risk and low-risk HPV was 6.0% and 2.8% respectively. Greater number of sexual partners was only associated with high-risk HPV (1.88; 95% CI: 1.22, 2.90) prevalence. In multi-variable models, residing in Mexico (1.66, 95% CI: 1.15, 2.40) and smoking (1.66, 95% CI: 1.13, 2.44) were significantly associated with high-risk HPV, and history of consistent gum bleeding (2.16; 95% CI: 1.35, 3.45) was significantly associated with low-risk HPV. Gender of the sexual partner did not alter the results for either high- or low-risk HPV endpoints. Different factors were independently associated with high- and low-risk oral HPV. Oral sexual behaviors were associated with high-risk HPV and oral health with low-risk HPV. High risk HPV prevalence differed by country of residence, highlighting the need for additional studies in multiple countries.
Bettampadi, D. Differences in factors associated with high and low risk oral HPV genotypes in men. The Journal of Infectious Diseases, jiaa693, https://doi.org/10.1093/infdis/jiaa693
—————————————————————————————————————————————————————————————————————
In a 2019 paper, researchers looked at more of the underlying details of the epidemic of oropharyngeal cancers in the US. While the incidence has soared in white men and gone up also in white women, it has actually decreased in black men and women. See Tota et al Evolution of the Oropharynx Cancer Epidemic in the United States: Moderation of Increasing Incidence in Younger Individuals and Shift in the Burden to Older Individuals. J Clin Oncol. 2019 Jun 20;37(18):1538-1546. doi: 10.1200/JCO.19.00370. Epub 2019 Apr 26.
—————————————————————————————————————————————————————————————————————
According to this 2021 paper, the incidence of oropharyngeal cancers caused by HPV are not expected to decline until after 2045 in the U.S. That’s because there are a large number of people who are already infected (because they have never been vaccinated), but have not yet developed cancer, and will do so during the next 24 years. Put another way, the benefits of the vaccinations on oropharyngeal cancer rates will only become evident after another two decades have passed. The incidence among younger people will decline before that time because a number of them have been vaccinated. Those who are 35 and over now can expect no decrease in oropharyngeal cancer rates.
Zhang, Y. et al Projected Association of Human Papillomavirus Vaccination With Oropharynx Cancer Incidence in the US, 2020-2045. JAMA Oncol. Published online September 2, 2021. doi:10.1001/jamaoncol.2021.2907
-
4) Has There Also Been a Big Spike in Oral HPV Cancers in Women?
- Yes, the number of these cancers has also increased markedly, though not as much as in men. The number or women with HPV-caused oropharyngeal cancers climbed from 2,409 in 1999 to 3,438 in 2015 (a 40 percent increase). The ratio of male:female HPV-caused oropharyngeal cancers was 2.9 to 1 in 1999, but climbed to 4.5 fold by 2015. The incidence of these cancers is growing much faster in men than women, and is thought to follow increases in oral HPV infections in men.
According to the CDC, in 2015, oropharyngeal cancers made up only 14% of all HPV-cancers in women. The most prevalent HPV-cancer in women is cervical cancer (48%), followed by anal cancers (18%), vulval cancers (16%), and vaginal cancers (3%). Contrast this with men, where oropharyngeal cancers made up 82% of all HPV-cancers in men, followed by anal cancers (12%) and penile cancers (6%). -
5) How Are HPV Strains Shared Between People?
- According to the CDC:
HPV is primarily spread by intimate skin to skin contact. You can be exposed to the virus by having oral, vaginal, or anal sexual contact with someone who is already infected. The virus can be transmitted by penetrative as well as non-penetrative sexual contact (genital-genital, oral-genital, anal-genital, oral-anal). Since many people have no symptoms of infection, it’s pretty common to become infected and to not even realize that has happened.
It had been thought that the hands can also transmit a genital, oral, or anal HPV infection. However, a new report in 2019 showed that the hands are actually a very unlikely source of viral transmission. Malagon et al Hand-to-genital and genital-to-genital transmission of human papillomaviruses between male and female sexual partners (HITCH): a prospective cohort study. The Lancet Infectious Diseases Feb. 2019 doi:10.1016/S1473-3099(18)30655-8
Most people will never develop symptoms of the infection as their immune systems will successfully eliminate the virus. However, some infected individuals will go on to develop either genital or anal warts, or to develop oral, anal, vaginal, vulval, penile, or cervical cancers. It can take years or even decades for these cancers to develop, making it very difficult to identify when a person actually became infected. Risk factors for catching HPV infections include an early age of first sexual intercourse, an increasing number of sexual partners, smoking, and having a compromised immune system.
Risk factors for catching HPV infections include:
Number of sexual partners. The more sexual partners you have, the more likely you are to contract a genital HPV infection. Having sex with a partner who has had multiple sex partners also increases your risk.
Age. Common warts occur mostly in children. Genital warts occur most often in adolescents and young adults.
Weakened immune systems. People who have weakened immune systems are at greater risk of HPV infections. Immune systems can be weakened by HIV/AIDS or by immune system-suppressing drugs used after organ transplants.
Damaged skin. Areas of skin that have been punctured or opened are more prone to develop common warts.
Personal contact. Touching someone's warts or not wearing protection before contacting surfaces that have been exposed to HPV — such as public showers or swimming pools — might increase your risk of HPV infection.
Source: Mayo Clinic
Risk factors specific for oral HPV infections include:
Oral sex. The prevalence of oral HPV infection was increased in subjects who had experience with oral sex as compared to those who did not.
Number of oral sex partners. Those with more oral sex partners had a higher incidence rate for HPV infection.
Smoking. This was significantly associated with oral HPV infections in both men and women
Source: See Shigeshi and Sugiyama Risk Factors for Oral Human Papillomavirus Infection in Healthy Individuals: A Systematic Review and Meta-Analysis J Clin Med Res. 2016 Oct; 8(10): 721–729. doi: 10.14740/jocmr2545w
People’s sexual practices, and how they are associated with HPV cancers, has been investigated in detail. The report concluded, “The number of oral sex partners remains a strong risk factor for HPV‐OPC; however, timing and intensity of oral sex are novel independent risk factors. These behaviors suggest additional nuances of how and why some individuals develop HPV‐OPC.”
You can read more about this study in this article from the NY Times: How Our Sex Habits May Affect Our HPV and Cancer Risk from Jan. 2021.
Drake, V.E. Timing, number, and type of sexual partners associated with risk of oropharyngeal cancer. Cancer https://doi.org/10.1002/cncr.33346. -
6) How Does The CDC Define “High Risk” Strains Of HPV?
- Any oral HPV: Oral rinse sample tested positive to one or more of the 37 HPV types listed under “All HPV types.”
High-risk oral HPV: Oral rinse sample tested positive to one or more of 14 high-risk HPV types (see definition) out of the 37 HPV types.
Any genital HPV in women: Vaginal swab sample tested positive to one or more of the 37 HPV types listed under “All HPV types.”
High-risk genital HPV in women: Vaginal swab sample tested positive to one or more of the 14 high-risk HPV types (see definition) out of the 37 HPV types.
Any genital HPV in men: Penile swab sample tested positive to one or more of the 37 HPV types listed under “All HPV types.”
High-risk genital HPV in men: Penile swab sample tested positive to one or more of the 14 high-risk HPV types (see definition) out of the 37 HPV types.
All HPV types (includes types detected by L1 consensus polymerase chain reaction): 6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 45, 51, 52, 53, 54, 55, 56, 58, 59, 61, 62, 64, 66, 67, 68, 69, 70, 71, 72, 73, 81, 82, 83, 84, 89, or IS39.
High-risk HPV types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, or 68.
Source: CDC Prevalence of HPV in Adults Aged 18–69: United States, 2011–2014 -
7) What Percentage Of Women In The US Have Cervical HPV Infections?
- It’s estimated that HPV infections are responsible for 90-99% or more of cervical cancer cases. It’s not clear if there are even any cases of cervical cancer that are not caused by HPV. Some doctors doubt that HPV-negative cervical cancer is possible. Maurie Markman, MD, editor-in-chief, OncologyLive®, and physician and president of Medicine and Science at Cancer Treatment Centers of America, said that the issue surrounding HPV-negative disease is that the HPV may simply not be found through testing, but is present. “If you're talking about the cervical cancer that we speak about, you can have the HPV found after very carefully searching, [even] if it's 1% [of HPV positivity] or less,” Markman said. “Some of this is definitional. The fact that you don't find it doesn't mean it isn't there.” Potential explanations for HPV-negative results include cervical cancers that are independent of high-risk HPV i.e. cervical cancers due to low-risk and intermediate-risk HPV, cervical cancers that lose HPV expression as the tumor grows, misclassified cancers, and poor HPV testing methods, including false-negative results.
How cervical cancers are caused by HPV is different from how oropharyngeal cancers are caused by HPV. This helps explain why the time frames for developing these cancers are different. In both men and women, the median age for developing HPV+ squamous cell carcinoma is around 61. In contrast, the median age for developing cervical squamous cell carcinoma is 50, although most cases are diagnosed in the 35 to 44 range.
This article explains how oropharyngeal and cervical cancers cause by HPV develop differently:
Martinelli, C. et al Molecular Mechanisms and Clinical Divergences in HPV‑Positive Cervical vs. Oropharyngeal Cancers: A Critical Narrative Review.
BMC Medicine (2025) 23:405 https://doi.org/10.1186/s12916-025-04247-z (FREE)
————————————————————————————————————————————————————————————————————————
There are over 200 different clinical tests that can be done to detect HPV infections. Most target the viral genetic material (either DNA or RNA). At least one targets the transcripts made by the virus, while others focus on the expression of genes contained within the virus. Choosing the right test is important in determining if one is, or is not positive for the virus, and if so, for which strain of virus.
————————————————————————————————————————————————————————————————————————
The prevalence of any cervical HPV infection is 26.8% for ages 14-59. 15.2% of women have are infected with high-risk (e.g. potentially cancer causing) strains of HPV, the most common being HPV16. The peak prevalence of cervical HPV infection is 44.8% in women ages 20-24, a few years following their sexual debut.
Reference: Guo T et al The Potential Impact of Prophylactic HPV Vaccination on Oropharynx Cancer. Cancer. 2016 August 1; 122(15): 2313–2323. doi:10.1002/cncr.29992.
The estimated lifetime risk for developing cervical cancer is only 0.68%, or about 1 in 147 women.
Howlader, et al SEER cancer statistics review, 1975-2009 (vintage 2009 populations). National Cancer Institute, https://seer.cancer.gov/archive/csr/1975_2009_pops09/.
New models of cervical cancer carcinogenesis suggest that HPV is necessary, but not sufficient, for the development of cervical cancer. The identification of a pathway contributing to cervical cancer involves activation of the YAP1 oncogene. See He et al A Human Papillomavirus-Independent Cervical Cancer Animal Model Reveals Unconventional Mechanisms of Cervical Carcinogenesis. Cell Reports 26, 2636–2650, 2019. r(s). https://doi.org/10.1016/j.celrep.2019.02.004
About 40% of pregnant women in the US have an HPV infection, and HPV could be detected in 10% of placentas. Only 7% of neonates had HPV at birth, and no infection persisted at 6 months.
Khayargoli, P.et al JAMA Pediatr. Published online May 22, 2023. doi:10.1001/jamapediatrics.2023.1283
———————————————————————————————————————————————————————————————————————————————
One notable recent finding is that there are significant differences in letting women in different ethnic groups know that they have been diagnosed with an HPV infection.
“White women are twice more likely to be told they have human papillomavirus (HPV) infection than Asian women and almost 3 times more likely than Black women.” In addition, “women born in the United States were 2.1 times more likely to receive a HPV diagnosis from a physician than women born in a foreign country, and women with a college education were 2.9 times more likely than women without a high school degree.
The findings do not mean that White, US-born, or college-educated women are more likely to contract HPV. It’s a communication issue.”
Hung M, et al. Health disparities associated with females reporting human papillomavirus infection in the United States. Women’s Health Rep. Published online July 15, 2021. doi:10.1089
Does the HPV vaccine really work to reduce cancer rates? Recent data says that it does:
As a result of the introduction of the HPV vaccine in 2006, we are starting to see declines in the prevalence of the HPV types that the vaccine targets. In one study, the prevalence of vaccine-type HPV decreased >90% in vaccinated women, demonstrating high effectiveness in a community setting, and >30% in unvaccinated women, providing evidence of herd protection.
See Kahn et al Substantial Decline in Vaccine-Type Human Papillomavirus (HPV) Among Vaccinated Young Women During the First 8 Years After HPV Vaccine Introduction in a Community. Clinical Infectious Disease 63, 1281 (2016) DOI: 10.1093/cid/ciw533
Also as a result of the introduction of the HPV vaccine in 2006, we are starting to see declines in the incidence of cervical pre-cancers both in those that are vaccinated as well as those who aren’t via herd immunity in both white and black women:
“In 10,206 cases, the proportion and estimated number of cases of HPV16/18-positive CIN2+ declined from 52.7% (1,235 cases) in 2008 to 44.1% (819 cases) in 2014 (P < 0.001). Declining trends in the proportion of HPV16/18-positive CIN2+ were observed among vaccinated (55.2%–33.3%, P < 0.001) and unvaccinated (51.0%–47.3%, P = 0.03) women; ages 18–20 (48.7%–18.8%, P = 0.02), 21–24 (53.8%–44.0%, P < 0.001), 25–29 (56.9%–42.4%, P < 0.001), and 30–34 (49.8%–45.8%, P = 0.04) years; CIN2 (40.8%–29.9%, P < 0.001) and CIN2/3 (61.8%– 46.2%, P < 0.001); non-Hispanic white (59.5%–47.9%, P < 0.001) and non-Hispanic black (40.7%– 26.5%, P < 0.001).”
See McClung et al Trends in Human Papillomavirus Vaccine Types 16 and 18 in Cervical Precancers, 2008– 2014 . Cancer Epidemiology, Biomarkers & Prevention DOI: 10.1158/1055-9965.EPI-18-0885
McClung and coworkers followed this up with a more recent study Declines in Vaccine-Type Human Papillomavirus Prevalence in Females Across Racial/Ethnic Groups: Data From a National Survey. J. Adolescent Health Volume 65, Issue 6, Pages 715–722, 2019. Their conclusions? “Within 10 years of vaccine introduction, 4vHPV-type prevalence declined 86% among 14- to 19-year-olds, with declines observed in non-hispanic whites, non-hispanic blacks, and Mexican-American females, and 71% among 20- to 24-year-olds, with declines in non-hispanic white and non-hispanic black females. These extraordinary declines should lead to substantial reductions in HPV-associated cancers.”
Finally, and most importantly, as a result of the introduction of the HPV vaccine in 2006, we are starting to see declines in the prevalence of cervical cancer in the young women first given the vaccine. The 4-year average annual incidence rates for cervical cancer in 2011–2014 were 29% lower than that in 2003–2006 (6.0 vs 8.4 per 1,000,000 people) among females aged 15–24 years, and 13.0% lower among females aged 25–34 years.
Guo et al Cervical Cancer Incidence in Young U.S. Females After Human Papillomavirus Vaccine Introduction. American Journal of Preventive Medicine Volume 55, Issue 2, 197–204, 2018. https://doi.org/10.1016/j.amepre.2018.03.013
In a study out of Finland, again based on the clinical trials of the HPV vaccine there, there was not a single case of ANY HPV+ cancer found in that cohort of 3,331 women given either the bivalent or the quadrivalent vaccine seven years after the trial began.
Luostarinen et al Vaccination protects against invasive HPV-associated cancers. Int. J. Cancer: 142, 2186–2187 (2018)
IMPORTANT NOTE: In Western developed countries, the cervical cancer incidence has been decreasing due to HPV vaccination and regular screening, as noted above.
However, cervical cancer is the fourth most common cancer worldwide, as screening is not widely done in many countries.
Cervical cancer is the most common form of cancer-related mortality in sub-Saharan African women, with researchers predicting a 50 per cent increase in cervical cancer mortality by 2040. Studies in Ugandan women have shown that different strains of HPV are associated with more aggressive types of cancer e.g. HPV 18-caused cervical cancers were more aggressive than HPV 16-caused cancers. -
8) Why Is The Incidence Of HPV Cancers Bimodal, With Peaks At 30-34 And 60-64?
- To visualize this bimodal peak in HPV infection, see Fig. 4 in Gillison ML et al Epidemiology of Human Papillomavirus–Positive Head and Neck Squamous Cell Carcinoma J. Clin. Oncol. 33, #29, 3235-3242 DOI: 10.1200/JCO.2015.61.6995
According to Guo T et al The Potential Impact of Prophylactic HPV Vaccination on Oropharynx Cancer Cancer. 2016 August 1; 122(15): 2313–2323. doi:10.1002/cncr.29992., “Explanations for the first peak include a surge in oral HPV infection after sexual debut and at peak sexual activity. The second peak may be attributed to potential reactivation of dormant infections with immunosenescence, increased HPV exposure in divorced or widowed populations, and/or increased rates of persistent infection which increase overall prevalence.”
These are interesting hypotheses, and there are others (e.g. rise of condom use as a result of the AIDS epidemic) but I don’t know of any data that really supports one idea over another regarding the second peak at age 60 to 64. I think it remains unexplained exactly why there are fewer cases of oropharyngeal cancer in those in the 35-59 year old age group. This may be a difficult question to answer epidemiologically.
A more recent study has shown that this bi-modal distribution of oral HPV types is much less pronounced than what was observed earlier, at least for all HPV strains. However, infection with cancer causing types still appear to be bimodal.
A number of multisite analyses have shown that oral and genital infections are in general poorly correlated and should be tested for separately. Indeed, an individual may have an infection at only one site, infections of different genotypes at genital and oral sites (con- current infection), or infections of the same genotype (concordant infection).
Brouwera, A.F. Multisite HPV infections in the United States (NHANES 2003–2014): an overview and synthesis. Preventive Medicine Volume 123, June 2019, Pages 288-298. https://doi.org/10.1016/j.ypmed.2019.03.040 -
9) Can HPV In One Part Of Your Body Migrate To Another?
- The answer to this question is probably not. Survivors of HPV cancers are at a slightly increased risk of developing a second HPV-caused cancer (see FAQ12 and FAQ17 below). This could indicate that the virus has spread in the body, but it could also mean that the person is infected with two different cancer-causing strains of HPV, and those infections just happen to be in separate places. The only way to really answer this question is to do genetic sequencing of the virus from different body sites, and see if the exact same sequence is found at multiple sites. Even then, this would not guarantee that the virus has spread, because the person could have been infected at multiple locations during the initial infection.
You can develop different HPV infections at different sites in your body. A study was done in men to look at their acquisition of HPV strains at different anatomic sites over time. The researchers “assessed samples obtained from 3,140 men enrolled in a longitudinal cohort for sequential genital to oral infection with one of nine HPV types (HPV 6, 11, 16, 18, 31, 33, 45, 52, 58); and then also sequential, same-type oral to genital infection. They observed a significantly higher incidence of an oral HPV infection among men with a prior genital infection of the same type for any of the 9 HPV types. Overall findings suggest that HPV infections at one site could raise the risk of a subsequent genital or oral HPV infection of the same type in men, stressing the relevance of vaccination to prevent all HPV infections.”
Dickey BL, et al Sequential acquisition of human papillomavirus infection between genital and oral anatomic sites in males. International Journal of Cancer July 7, 2021 -
10) Are Different Strains of HPV Causing Cancer In Different Places Globally?
- No. While HPV 16 is the predominant strain in all countries where these studies have been done, the percentage of other strains differs markedly. HPV was found in 99.7 percent of cervical cancer samples analyzed worldwide. See Waldboomers et al Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 189, 12-19, 1999.
The graphic below shows type-specific human papillomavirus (HPV) prevalence for most frequent HPV types by geographical region. Type-specific HPV prevalence is weighted by study size and standardized by the world's geographical structure. It’s Figure 3 from Bruni, L. et al Cervical Human Papillomavirus Prevalence in 5 Continents: Meta-Analysis of 1 Million Women with Normal Cytological Findings. The Journal of Infectious Diseases, Volume 202, Issue 12, 15 December 2010, Pages 1789–1799, https://doi.org/10.1086/657321. FREE paper.
As you can see from the graphic below, different strains of HPV have different prevalences around the world. It turns out that different strains of HPV are also associated with different levels of aggressiveness of cervical cancers. Put another way, some strains of HPV are more associated with aggressive cancer than other strains. Mechanistically, this is thought to be due to different levels of expression of the cancer causing genes in HPV, E6 and E7. For example, the HPV 18 strain was considered to result in more aggressive cancers than HPV 16 in Ugandan women with cervical cancer.
Gagliardi, A. et al Analysis of Ugandan cervical carcinomas identifies human papillomavirus clade–specific epigenome and transcriptome landscapes. Nature Genetics 52, 800–810, 2020
Van Doorslaer, K. and Burk, R.D. Evolution of Human Papillomavirus Carcinogenicity. Adv Virus Res. 2010 ; 77: 41–62.
—————————————————————————————————————————————————————————————————
One other factor that is at play here is the bacterial composition of the surface of the cervix. It appears that different strains of bacteria that live on the cervix (known collectively as the microflora) can affect the ability of the body to eliminate (or not) the virus following infection. The work is in it’s early stages, and you can read about it here: McDermott, Amy. Microbiome insights open new avenues to treat HPV. Proceedings of the National Academy of Sciences. doi: https://doi.org/10.1073/pnas.2304645120 https://www.pnas.org/doi/10.1073/pnas.2304645120 -
11) Do Partners of Oral HPV-cancer Patients Have Higher Levels of Oral HPV?
- No. HPV status was looked at in the female and male partners of men who had HPV+ oral cancers. The researchers found that the partners had comparable oncogenic oral HPV prevalence (i.e. they were HPV 16+) compared with members of the general population of the same age (1.2% v 1.3%). No precancers or cancers were identified during partner oral cancer screening examinations either.
Reference: D’Souza et al Oral human papillomavirus (HPV) infection in HPV-positive patients with oropharyngeal cancer and their partners. J Clin Oncol. 10, 2408-15, 2014. doi: 10.1200/JCO.2014.55.1341. -
12) Are HPV-cancer Survivors At Risk Of Developing A Second HPV Cancer?
- Unfortunately, yes. Survivors of HPV-associated cancers are at an increased risk of developing HPV second primary cancers (HPV-SPCs). Among both women and men, the risk of developing HPV-SPC at the original cancer site was higher than that of developing HPV-SPC at a different cancer site. Among women with index vaginal, vulvar, and anal cancers, the risk for all HPV-SPCs remained high. The HPV-SPC risk was lowest among women with index cervical cancer. Among men, the oropharyngeal SPC risk was elevated after index penile and anal cancers. Given the large difference in the HPV-SPC risk between survivors of HPV-associated cancers and that of non–HPV-associated cancers, it is likely that persistent HPV infection contributes to the development of HPV-SPCs among survivors of HPV-associated cancers.
Reference: Suk et al Trends in Risks for Second Primary Cancers Associated With Index Human Papillomavirus–Associated Cancers. JAMA Network Open. 2018;1(5):e181999. doi:10.1001/jamanetworkopen.2018.1999 (FREE ARTICLE)
If you’ve been treated for oropharyngeal cancer, what is the likelihood that your disease may spread after treatmentThis was looked at in a recent study from Denmark. The patients diagnosed with oropharyngeal squamous cell carcinoma (OPSCC) from 2000 to 2014 were treated with curative intent. Tumors were defined as HPV-positive when they were both HPV-DNA and p16-positive.
Results: The cohort consisted of 1244 consecutive patients with OPSCC of which 288 patients (23%) experienced recurrence. Of these patients, the majority (n = 197/1244; 16%) experienced loco-regional recurrence (LRR) and the remaining (n = 91/1244; 7%) had distant recurrence (DR). Significantly more HPV-negative patients experienced recurrence (n = 170/486; 35%) compared to HPV-positive patient (n = 112/726; 15%). DR occurred for both groups predominantly to the lung (n = 63/91; 69.2%) followed by the liver and bone. Factors influencing the risk of LRR included gender, T-classification, and HPV-status. The same variables influenced risk of DR in addition to the UICC-8 classification, N-classification, pack years of smoking, and performance status. HPV-status was the strongest risk factor for LRR and DR.
Conclusion: LRR and DR occur significantly less often in HPV-positive patients compared with HPV-negative patients. HPV-status is an independent and strong predictor of recurrence. DR most commonly occurs to the lungs, irrespective of HPV-status.
Gronhoj, c. et al Pattern of and survival following loco-regional and distant recurrence in patients with HPV+ and HPV− oropharyngeal squamous cell carcinoma: A population-based study. Oral Oncology Volume 83, August 2018, Pages 127-133. -
13) What Happens More Easily: Men Infect Women With HPV, or Women Infect Men?
- The available data indicates it’s a much more efficient process (3 times as much) for women to give the virus to men rather than vise-versa. In addition, according to the paper, “The penis shaft was the primary source of transmission to the cervix; the cervix and urine were the primary sources of infection to male genitals. Sexual transmission also involved the scrotum, the anus of women, and the hands of both sexes. The oral cavity and semen were not involved in transmission. The anus of women was both a major source and target of heterosexual transmission. We observed consistency between penis-to-female anus transmission and reported anal intercourse during the corresponding period.”
Source: BY Hernandez et al Transmission of Human Papillomavirus in Heterosexual Couples. Emerg Infect Dis. 2008 Jun; 14(6): 888–894. doi: [10.3201/eid1406.070616.2]
This data was recently backed up by another report. However, this data varied greatly from study to study, and also appeared to vary with the strains of HPV chosen. In short, it’s complicated.
Directionality of genital human papillomavirus infection transmission within heterosexual couples: A systematic review and meta-analysis. Balaji, R. et al. The Journal of Infectious Diseases, jiaa302, https://doi.org/10.1093/infdis/jiaa302. -
14) Do Men And Women Generate Anti-HPV Antibodies Equally Well?
- It appears there is a big difference here. Researchers looked at the prevalence of antibodies to HPV strains 16 and 18 (these are cancer causing strains) and strains 6 and 11 (that can cause genital warts, not cancer) in three groups that have had sex, but had not been vaccinated against HPV. The groups were women, men who had sex with men i.e. gay or bisexual (MSM), and men who had sex with women (MSW). Results of the study showed that the level of antibodies to HPV among MSM and women were comparable at 42.6% and 37.1%, respectively. In contrast, the ability to generate antibodies to HPV was greatly reduced among MSW at only 13.2%. Additionally, the researchers found that the ability to generate antibodies increased with the number of lifetime sexual partners in all three groups. Why the gender differences? Researchers believe it is due to the nature of the tissues where the infections take place. Antibodies are more likely to be generated after exposure at non-keratinized (mucosal) surfaces compared to keratinized epithelium. Thus, if infection occurs in the anus, or inside the vagina, these represent exposure at mucosal surfaces. An infection on the penis would be an example of an infection on a keratinized epithelial surface. Mucosal tissues are those that are likeliest to spread infection.
Source: Lewis RM, et al. Seroprevalence of human papillomavirus 6/11/16/18 among self-identified gay/bisexual men who have sex with men, men who have sex with women, and females, United States, 2003–2010. Clin Infect Dis. 2018; 10.1093/cid/ciy1002.
What’s unclear to me in all of this is antibody prevalence related to oropharyngeal infection (also a mucosal surface). Thus, men who have vaginal sex with women are relatively resistant to infection on the keratinized surface of the penis. In contrast, men who perform oral sex on women should be quite prone to infection with HPV because of the oral mucosa in their mouths. Why this doesn’t translate into the generation of antibodies in men is unclear to me. According to a different source, “the fact that infections in other mucosal sites of the body (e.g. the mouth) also elicit antibody responses that cannot be distinguished from those arising in the anogenital area.” Separating out responses to oral vs. anogenital exposure as measured via serum antibody levels seems a very complex undertaking that is unlikely to provide a clear answer because sexual behavior differs widely between individuals.
IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 90. IARC Working Group on the Evaluation of Carcinogenic Risk to Humans.
Lyon (FR): International Agency for Research on Cancer; 2007. -
15) How Old Are People When They're Diagnosed With An HPV-caused Cancer?
- With one significant exception, most of the cases of HPV-caused cancers are found in older adults.
The exception is cervical cancer, a disease that hits women during their reproductive years. Here’s the data from the CDC website:
The median age at diagnosis (the age at which half of cancer patients were older and half were younger), is:
49 years for HPV-associated cervical cancer.
67 for HPV-associated vaginal cancer.
66 for HPV-associated vulvar cancer.
69 for HPV-associated penile cancer.
62 among women and 59 among men for HPV-associated anal cancer.
62 among women and 61 among men for HPV-associated oropharyngeal cancers.
The graphs below (again, from the CDC) illustrate the trends more clearly. Note that the scale on the Y axis is different on the two graphs. The other key point is that the highest incidence rate of all HPV-caused cancers is associated with oropharyngeal cancers in men. The peak rate is 2.5X as large as the peak rate for cervical cancer in women. -
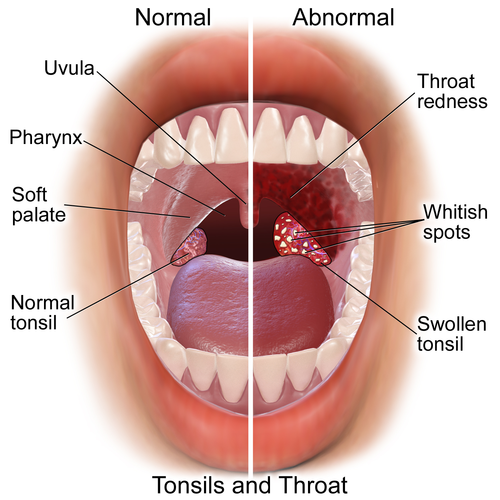
16) Does Tonsillectomy Prevent HPV-caused Tonsil Cancers?
- Tonsillectomy reduces the chances of getting HPV-cancers, but does not eliminate it. This is because you have multiple sets of tonsils, including the lingual tonsils and the palatine tonsils (the ones removed in a standard tonsillectomy), each of which can be a site of HPV-caused cancer. In addition, failure to extract the tonsillar crypts during surgery can leave that remaining tonsil fragment at risk of HPV infection, and later cancer.
Source: Memorial Sloan Kettering Cancer Center
Tonsillectomy does NOT prevent the development of tonsil cancer, but it did reduce the number of cases of tonsil carcinoma diagnosed before age 60 by 85%, and any tonsil carcinoma by 60%. According to the authors, “This observation is made with caution. Tonsillectomy is not a surgical procedure to be discounted and can lead to both minor and major complications, including death. Careful consideration of the relatively low incidence of oropharyngeal carcinoma, potential morbidity and mortality of tonsillectomy, and promising potential impact of the prophylactic HPV vaccine is warranted.”
Not surprisingly, tonsillectomy does NOT prevent other HPV-caused oropharyngeal cancers (or HPV-caused cancers in other tissues) from developing. This fact, coupled with the surgical risks of and expenses of tonsillectomy, are why I don’t expect to find anyone proposing to do tonsillectomies prophylactically to prevent tonsil tumors.
Fakhry et al The Impact of Tonsillectomy upon the Risk of Oropharyngeal Carcinoma Diagnosis and Prognosis in the Danish Cancer Registry. Cancer Prevention Research, 1-7, 2015 doi: 10.1158/1940-6207.CAPR-15-0101
This photo may be helpful: -
17) Do Pre-Cancerous HPV Lesions Increase Your Risk Of Developing Cancer?
- Yes they do, according to a Scottish study: “All cases of pre-invasive penile, anal, vulval, and vaginal disease diagnosed in 1990-2015 were identified within the NHS pathology databases in the two largest NHS health boards in Scotland.” “Among 69714 females in Scotland diagnosed with CIN3 (890360.9 person-years), 179 developed non-cervical HPVaC. CIN3 cases were at 3.2-fold (95% CI: 2.7 to 3.7) increased risk of developing non- cervical HPVaC, compared to the general female population. Among 1235 patients diagnosed with non-cervical pre- invasive disease (9667.4 person-years), 47 developed HPVaC. Individuals with non-cervical pre-invasive disease had a substantially increased risk of developing HPVaC - 15.5-fold (95% CI: 11.1 to 21.1) increased risk for females and 28-fold (11.3 to 57.7) increased risk for males. We report a significant additional risk of HPV-associated cancer in those have been diagnosed with pre-invasive HPV- associated lesions including but not confined to the cervix.”
I didn’t find this result surprising because they’re looking at a population of patients that has already shown itself to be incapable of fighting off their HPV infections. As a result, I’d expect this group to have a much higher incidence of HPV-caused cancers than the general population.
Source: Kavanagh et al Increased risk of HPV-associated genital cancers in men and women as a consequence of pre-invasive disease. Int J Cancer. 2019 Jan 16 -
18) What's the Lifetime Risk Of Developing An HPV-cancer?
- For individuals not vaccinated against HPV, the cumulative risk of developing an HPV-associated cancer was 1.4% in white women, and about 0.98% in white men. Thus, about 1 in 71 white women will develop one of these cancers, and about 1 in 100 white men will. If we focus just on cervical cancer, the estimated lifetime risk for developing cervical cancer is only 0.68%, or about 1 in 147 women.
Howlader, et al SEER cancer statistics review, 1975-2009 (vintage 2009 populations). National Cancer Institute, https://seer.cancer.gov/archive/csr/1975_2009_pops09/.
For individuals not vaccinated against HPV, the cumulative risk of dying from an HPV-associated cancer was
0.24% for females and 0.20% for males, where Non-Hispanic Black individuals faced the highest burden for both sexes (i.e., 0.32% and 0.25%, respectively). Thus, about 1 in 417 white women will die one of these cancers, and about 1 in 500 white men will.
The paper below contains this data, along with data for other racial groups. It also estimates the risks following immunization with the bivalent and nonavalent HPV vaccines.
Data from: Burger et al Racial and ethnic disparities in human papillomavirus (HPV)- associated cancer burden with first- and second-generation HPV vaccines. Cancer. 2016 July 1; 122(13): 2057–2066. doi:10.1002/cncr.30007. -
19) Does The HPV Vaccine Increase Your Risk Of Developing Diabetes?
- No. Researchers examined all potential cases of type 1 diabetes that were identified from members of Kaiser Permanente Northern California (KPNC) aged 11-26 years at any time from June 2006 to December 2015. The analysis of DM1 included 911,648 people. No increased risk was found for the development of DM1 following HPV vaccination.
Reference: Klein et al Long term risk of developing type 1 diabetes after HPV vaccination in males and females. Vaccine, March 05, 2019 -
20) How Are HPV Head And Neck Cancers Classified?
- This is a developing story with some important potential clinical applications. In short, while most HPV+ H&N cancer patients do well with standard treatments, a small percentage don’t (they are more similar to HPV negative H&N cancer patients in this regard). Researchers at MD Anderson Cancer Center examined the expression of a large collection of cellular proteins that interact with HPV to figure out what distinguishes those patients who respond well from those who don’t. In the end, they found a subset of 38 genes whose expression correlated with outcomes to treatment. How is this useful? Two implications are is that it may eventually enable doctors to identify patients before treatment who are NOT likely to respond to standard therapies, and thereby shunt them into different therapeutic regimens. It may also enable doctors to ID patients who are likely to have good outcomes with standard therapy for de-escalation treatments. The hope is that this will enable patients to get lower doses of damaging radiation (and therefore experience less tissue damage), yet still achieve good survival outcomes. This will need to be established in future clinical trials.
Here are the references for those wanting to learn more:
Gleber-Netto et al. Variations in HPV function are associated with survival in squamous cell carcinoma. JCI Insight. 2019;4(1):e124762. https://doi.org/10.1172/jci.insight.124762. FREE paper
This paper is a more readable explanation of what the paper above is suggesting:
R. Hepp New Biomarker Reveals HPV Function in Head & Neck Cancers. Oncology Times: March 5, 2019 - Volume 41 - Issue 5 - p 17–18 doi: 10.1097/01.COT.0000554320.58842.75
—————————————————————————————————————————————————————————————————————————
In a separate study, researchers did retrospective genomic analyses on samples from patients with HPV+ and HPV- oropharyngeal cancers (OPSCC), so they had outcomes data on how the patients fared. Overall, HPV negative status, soft palate location, and smoking were associated with poorer outcomes in OPSCC. HPV- OPSCC were genetically distinct from the HPV+ OPSCC. Risk-stratification could be further refined based on the mutational signature. HPV+ OPSCC patients with NOTCH1 mutations, and HPV- OPSCC patients with SOX2 mutations, each fared significantly worse. Note: this analysis focused on looking at mutations in genes that might be predictive of differential outcomes, whereas the study above was focused on expression of genes.
Dogan, S. et al. Identification of prognostic molecular biomarkers in 157 HPV-positive and HPV-negative squamous cell carcinomas of the oropharynx. Int J Cancer. 2019 May 16. doi: 10.1002/ijc.32412
Note that the presence of HPV is associated with greater survival not just for oropharyngeal head and neck cancers, but also for non-oropharyngeal head and neck cancers.
Wookey, V.B. et al HPV Status and Survival in Non-Oropharyngeal Squamous Cell Carcinoma of the Head and Neck. ANTICANCER RESEARCH 39: 1907-1914 (2019)
—————————————————————————————————————————————————————————————————————————
In yet another study, researchers were able to once again divide the responsiveness to chemo/radiation of HPV+ oropharyngeal cancer patients. They found the two distinct subtypes directly correlated with patient outcomes. Tumors with low NF-kB activity were associated with worse prognosis, while tumors with high NF-kB activity were associated with a better prognosis.
The subtypes identified by high or low NF-kB activity were remarkably different from one another, from the genes that were mutated in the cancers, factors driving the mutations, the number of mutations per cancer, HPV gene expression, HPV integration, gene methylation, and infiltration of certain immune cells into the tumor.
This data suggests that it might be possible to treat patients differently depending on the NF-kB activity of their tumors. It's possible that those with high NF-kB activity might need less treatment than low with low levels of this activity. This will need to be confirmed in clinical trials.
Press release: Two Subtypes of HPV-associated Head and Neck Cancers Predict Treatment Outcomes
Science paper: Scharank, T.P. Noncanonical HPV carcinogenesis drives radiosensitization of head and neck tumors. PNAS July 31, 2023. 120 (32) e2216532120. https://doi.org/10.1073/pnas.2216532120 -
21) Are Head And Neck Cancer Patients At Risk Of Developing Strokes (Radiation)?
- Maybe. The authors of the paper below concluded that HPV-positive status is associated with an increased risk of stroke or transient ischemic attack following radiation treatment for head and neck cancer. The authors themselves raise some caveats regarding this in terms of both how the patients were chosen for the analysis as well as which ones were available for follow up. I had some reservations about the conclusions drawn. First, there is no comparison (i.e. a control group) with a group that matched the H&N cancer patients. How many "normal" people (people with and without HPV infection, but no cancer) would have had strokes or TIAs over that same time period? Similarly, how would cancer patients that got radiation at some other location (e.g. prostate) compare to this group? Is it the radiation, where the radiation goes, or something else? Hard to say here. I also noticed that there was a higher proportion of men in the HPV-positive group, and maybe the increased stroke/CVE risk simply reflects having more men in that group. Finally, I'm not sure how actionable this data is. After all, no one would turn down the radiation therapy if it was needed just to have a lower risk of stroke/CVE.
Addison, D. et al Human Papillomavirus Status and the Risk of Cerebrovascular Events Following Radiation Therapy for Head and Neck Cancer. J Am Heart Assoc. 2017;6:e006453. DOI: 10.1161/JAHA.117.006453. (FREE paper) -
22) Do Oral And Genital HPV Infections Correlate With Each Other?
- The answer is no. A number of multisite analyses have shown that oral and genital infections are in general poorly correlated and should be tested for separately. Indeed, an individual may have an infection at only one site, infections of different strains at genital and oral sites (con-current infection), or infections of the same strains (concordant infection). Put another way, people with genital HPV infections may, or may not have oral infections. People with oral infections may, or may not, have genital infections. And people with both infections may easily have different HPV strains at the two sites, suggesting that they were acquired at different times and from different individuals.
Brouwera, A.F. Multisite HPV infections in the United States (NHANES 2003–2014): an overview and synthesis. Preventive Medicine Volume 123, June 2019, Pages 288-298. https://doi.org/10.1016/j.ypmed.2019.03.040
On a separate note, a recent report indicates that penile circumcision reduced the incidence and the persistence of HPV infections in men.
Smith, J.S. Male Circumcision Reduces Penile HPV Incidence and Persistence: A Randomized Controlled Trial in Kenya. Cancer Epidemiology, Biomarkers & Prevention. June 2021 Volume 30, Issue 6. DOI: 10.1158/1055-9965.EPI-20-1272 -
23) What Percentage of Cervical Cancer Cases Are Caused By HPV Infection?
- The numbers cited usually vary because they reflect the percentage of cervical cancer cases caused by different strains, and by the fact that the different HPV vaccines covered different numbers of strains. Let’s look at this by vaccine type:
The bivalent HPV vaccine (Cervarix) prevents infection by HPV strains 16 and 18. These are the most prevalent strains, and account for about 70% of cervical cancer cases.
The quadrivalent HPV vaccine Gardasil prevents infection by these same two HPV strains, plus two additional strains that cause genital warts. Gardasil should therefore be equivalent to Cervarix in preventing about 70% of cervical cancers.
The nonavalent HPV vaccine Gardasil 9 prevents infection by HPV strains 16 and 18, as well as cancer causing strains 31, 33, 45, 52, and 58. These seven strains account for a total of 88% of cervical cancers.
HPV strains 35, 59, 56, 51, 39, 73, 68, and 82 are NOT covered by the vaccine, and account for an additional 7% of cervical cancer cases. Cumulatively, all of these HPV strains (including 16.18, 31, 33, 45, 52, and 58) cause about 95% of cervical cancers. The remaining 5% are either caused by other, unidentified strains of HPV, or by something else entirely.
See Table 2 in Crosbie et al Human papillomavirus and cervical cancer. The Lancet 382 (9895) 2013. FREE download. -
24) Is Poor Oral Health Associated With Survival In H&N Cancer Patients?
- Yes it is, but the subject is complicated. That’s because poor oral health can be associated with poverty (leading to fewer dental visits), which is turn may delay the detection of oral cancers, leading to worse patient outcomes. In addition, poor oral health may contribute to changes to the oral microbiome via the presence of dental/oral inflammation or immune responses, or due to failure to brush teeth properly or consistently. The issues here are complex and can be difficult to separate out.
Farquhar et al Poor Oral Health Affects Survival in Head and Neck Cancer Oral Oncol. 2017 October ; 73: 111–117. doi:10.1016/j.oraloncology.2017.08.009. -
25) Are Men Who Have Sex With Men Taking PrEP At High Risk For Catching HPV?
- Yes. A new French study showed that while an increase in PrEP (pre-exposure prophylaxis to prevent HIV infection) can lead to a sharp decline in new HIV diagnoses, new cases of sexually transmitted infections (STIs) are still prevalent. PrEP can lead to an increase in sexual behaviors such as condomless anal intercourses with different partners, adding to the risk for anal STIs such as chlamydia, syphilis, gonorrhea, and HPV among MSM taking PrEP.
Investigators studied 61 MSM who had not received an HPV vaccine. The mean age was 36.1 years and about 1 in 3 men were in a stable relationship. About 72% reported having had sexual intercourse with at least 10 partners in the last 12 months, and nearly 30% reported at least 50 partners in that time. In addition, 21.3% of participants reported always using a condom during sex, 75.4% reported inconsistent use of condoms during sex, and 3.3% reported never using condoms during sex.
“Among study participants, 57 (93.4%) had anal HPV infection, including 50 (81.9%) participants with HR-HPV that can lead to HPV-related cancers. Investigators found anal infection with multiple HPV genotypes in 73.8% of participants and multiple HR-HPV infections containing an average of 3.1 HR-HPV genotypes per anal specimen in 44.3% of the MSM in the study. HR-HPV type 33 was the most prevalent genotype, followed by HPV-42, HPV-53, HPV-51, HPV-6, and HPV-70. Although all age groups had high rates of HPV infection, 100% of participants older than 50 years had HPV and rates of HR-HPV were highest in MSM ages 19 to 29 years.” “MSM reporting condomless receptive anal intercourse were 10.4-fold more likely to have anal HPV infection than those having exclusively insertive anal intercourse,” the research team added. “These findings confirm that the risk of anal STIs acquisition is strongly associated with the sexual behavior and the number of sexual partners in MSM population.”
Mboumba Bouassa, R.-S. et al High prevalence of anal and oral high risk-human papillomavirus in HIV-negative French men who have sex with men uptaking pre-exposure prophylaxis. Open Forum Infectious Diseases, ofz291, https://doi.org/10.1093/ofid/ofz291. FREE download. -
26) What Are The Five Year Survival Rates For HPV Cancers?
- I’ve provided some general numbers below. Keep in mind that every cancer case is different, and one cannot estimate this number for any particular case from the averages below. The data was compiled from the cancer.net website of the American Society for Clinical Oncology. Note that these are overall values for these types of cancers caused by HPV and any other causes. HPV causes nearly all cases of most of these cancers except for oropharyngeal cancer (where it makes up about 70% of cases), which is also caused by smoking and excessive alcohol consumption:
Note: There is a significant survival advantage in those who are diagnosed with HPV-positive tumors oropharyngeal cancers compared to HPV-negative oropharyngeal cancers. However, this survival advantage is only seen in oropharyngeal, laryngeal and hypopharyngeal HPV-positive tumors. There are no survival advantages associated with having HPV for other head and neck cancers, such as nasopharyngeal cancers.
Sahovaler, A. et al Survival Outcomes in Human Papillomavirus–Associated Nonoropharyngeal Squamous Cell Carcinomas: A Systematic Review and Meta-analysis
JAMA Otolaryngol Head Neck Surg. 2020;146(12):1158-1166. doi:10.1001/jamaoto.2020.3382
HPV+ penile cancer cases also show a survival advantage over HPV- cancers:
Chennamadhavuni A. Prognostic significance of human papillomavirus (HPV) in penile cancer: A National Cancer Database (NCDB) study. ASCO Genitourinary Cancers Symposium, 11-13 February 2021. -
27) Do Nuns Get Fewer Cases Of Cervical Cancer Than Other Women?
- It’s a bit difficult to find reliable data on this, but this appears to be true.
Much of what I could find is summarized below:
In mid-19th century Verona, Italy, Dr. Domenico Rigoni-Stern observed that uterine cancer, while relatively common in women living in the city, but was quite rare in the Catholic nuns who lived in the convents in the countryside. What accounted for this difference? Further investigation revealed that the risk of cervical cancer correlated with the number of sexual partners a woman had. Prostitutes had a relatively high risk of contracting the disease, married women in town had a moderate risk, and the celibate nuns only rarely had a case. This epidemiological profile strongly suggested that a sexually transmitted agent played an important role in the development of cervical cancer. Many sexually transmitted diseases were suspected of being the cause of this, but eventually it was tied to papilloma virus infection.
Source: DiMaio, D. Nuns, Warts, Viruses, and Cancer. YALE JOURNAL OF BIOLOGY AND MEDICINE 88 (2015), pp.127-129.
“Several investigators during the last two decades have confirmed Rigoni-Stern's observations concerning the rarity of uterine cervix cancer among nuns. Gagnon examined the medical files from many convents of French-Canadian nuns, covering an annual average of 13,000 women over a 20-year period, and found 14 cases of corpus cancer but none of the cervix. He then reviewed the pathologic archives of several hospitals and identified three cervical cancers compared with 19 corpus cancers among nuns. Finally, he made an ad hoc survey of four religious orders, with an average annual population of 3280 women whose medical histories over the previous 25 years were documented, and found a total of 222 cancers, 7 of which involved the uterine corpus and none, the cervix. Gagnon was impressed not only by the small absolute number of cervix uteri carcinomas among the nuns in these studies but also by their infrequency relative to corpus cancer, a reversal of the pattern usually observed. He attributed this to the rarity of chronic cervicitis, which he regarded as a major carcinogenic factor in virginal women.
In another investigation, Towne diagnosed cervical cancer in 3 nuns among 3083 seen in her private medical clinic and 3 others over a 20-year period in several large religious communities of about 10,000 women. Although she concluded that cervical malignancy can develop in women without regard to virginity or parity, the unusually low rate of cervical cancer, both absolute and relative, to that of corpus cancer is apparent.”
Quote from Priore, G, Glob. libr. women's med., Epidemiologic Aspects of Uterine Cervix Cancer, (ISSN: 1756-2228) 2008; DOI 10.3843/GLOWM.10225 Under review - Update due 2019.
In a separate study from 1969, Fraumeni, J.F. et al Cancer Mortality Among Nuns: Role of Marital Status in Etiology of Neoplastic Disease in Women. JNCI: Journal of the National Cancer Institute, Volume 42, Issue 3, Pages 455–468, https://doi.org/10.1093/jnci/42.3.455. The abstract reports that nuns do have a greatly reduced frequency of cervical cancer.
—————————————————————————————————————————————————————————————————————
The story does NOT end here. There is data showing that nuns are indeed at risk of developing cervical HPV infections. Is that because they're having sex? Not necessarily.
From a report from GAVI on HPV prevalence in nuns in Ghana:
"A recent initiative to offer free HPV testing for 10,000 women across Ghana and Nigeria provided Effah and his colleagues with an opportunity to screen this group of women. “Our main aim was to offer cervical cancer prevention services to a group at risk of cervical cancer that might have been ignored,” he said. With the permission of the Mother Superiors, they visited convents in the Greater Accra, Volta and Central regions of Ghana, and offered nuns the opportunity to self-collect cervical samples for HPV testing, under the supervision of a trained nurse. One hundred and five women did so, of whom 25 tested positive for high-risk HPV – a prevalence of 23.8%. This HPV-positivity rate is similar to that of the general Ghanaian population.
Those nuns who tested positive were offered Pap smears and a diagnostic procedure called a colposcopy to check for abnormal cells, with clinically relevant changes detected in two of them. However, follow-up tests suggested they were healthy. “This study highlights the need to include nuns in general cervical precancer screening programmes in Ghana, despite the historical and anecdotal perspective that cervical cancer is rare among them,” said Effah.
Non-sexual transmission
Although the nurses that screened the nuns didn’t ask them about their sexual histories, and it is possible that they acquired the virus through sexual contact, there are other ways through which they could have got the infection. Though relatively rare, HPV can be transmitted vertically from mother to child during delivery, as the baby passes through the genital tract. “We see many cases of women with genital warts and children (girls and boys) with vulval or anal warts,” said Effah. “What proportion of these is from vertical transmission needs to be studied, especially in a country like Ghana that has never started a national HPV vaccination programme.” Another means of non-sexual HPV transmission could be the use, or sharing of, bulb syringes for enemas – where liquid is injected directly into the rectum to relieve constipation, or as a remedy for various ailments, according to traditional west African medicine. “The use of bulb syringes (bentua) is common in Ghana and in many families the bulb syringes are shared by family members, including children,” said Effah.
Earlier studies have shown that the virus can survive on inanimate objects, including toilet seats, medical equipment and bathroom surfaces. HPV has also been detected on people's fingertips, raising the possibility of them infecting their own genitals – although this has not been proven." -
28) What's The Status Of Dose-Deescalation Studies For H&N Cancer Patients?
- These studies are coming along. Data from a phase II trial was published in August 2019. According to the abstract, the goal of the study was to determine if dose de-escalation (from 60 to 66 Gy to 30 to 36 Gy) of adjuvant radiotherapy (RT) for selected patients with human papillomavirus–associated oropharyngeal squamous cell carcinoma could maintain historical rates for disease control while reducing toxicity and preserving swallow function and quality of life (QOL).“ Acccrual was from September 2013 to June 2016 (N = 80; cohort A, n = 37; cohort B, n = 43). Median follow-up was 36 months, with a minimum follow-up of 25 months. The 2-year locoregional tumor control rate was 96.2%, with progression-free survival of 91.1% and overall survival of 98.7%. Rates of grade 3 or worse toxicity at pre-RT and 1 and 2 years post-RT were 2.5%, 0%, and 0%. Swallowing function improved slightly between pre-RT and 12 months post-RT, with one patient requiring temporary feeding tube placement. Conclusion from this trial: Aggressive RT de-escalation resulted in locoregional tumor control rates comparable to historical controls, low toxicity, and little decrement in swallowing function or QOL”. Hopefully this data will be replicated in the phase III trial.
Ma, D. et al Phase II Evaluation of Aggressive Dose De-Escalation for Adjuvant Chemoradiotherapy in Human Papillomavirus–Associated Oropharynx Squamous Cell Carcinoma. J. Clinical Oncology 37, no. 22 (August 1 2019) 1909-1918. https://doi.org/10.1200/JCO.19.00463
This is a topic that gets considerable debate in the oncology community. It’s well established that conventional treatments in treating these oral cancers using chemotherapy and radiation are very toxic and can be very debilitating for patients quality of life. The other side of the coin is that these treatments can be curative, but often do so at a substantial cost to the patient. There’s hope, backed up by numerous ongoing clinical trials, that the doses of chemotherapy and radiation can be reduced so that there is less harm to the patient, but at the same time preserving excellent cure rates.
I’m not a doctor, and even if I was, the decision to try dose de-escalation therapy needs to be decided on a case by case basis. For those of you who want to dive deep into the arguments on both sides, check out this article, preferably with your doctor:
Wirth et al Point/Counterpoint: Do We De-escalate Treatment of HPV-Associated Oropharynx Cancer Now? And How? 2019 ASCO EDUCATIONAL BOOK https://doi.org/ 10.1200/EDBK_ 238315 FREE Download
——————————————————————————————————————————————
Here’s another editorial about the various trials that are being done in dose de-escalation therapy, and I’ll share one thought from the article: “The landscape of treatment options for HPV-positive OPSCC somewhat mirrors that for low-risk prostate cancer—so many options, all of them seemingly promising, making the decision-making process incredibly confusing and difficult. ”
Chundury, A. et al. Radiation Dose De-Escalation in HPV-Positive Oropharynx Cancer: When Will It Be an Acceptable Standard of Care? J. Clin. Oncol. 2021 FREE Download 10.1200/JCO.20.03128
This editorial follows the publication of this article: Yom, S.S. et al Reduced-Dose Radiation Therapy for HPV-Associated Oropharyngeal Carcinoma (NRG Oncology HN002). DOI: 10.1200/JCO.20.03128 Journal of Clinical Oncology 2021. FREE Download
——————————————————————————————————————————————
Some good news to share from the "radiation dose-deintensification" trials for HPV-caused head and neck cancers. Results have just been published for a phase II trial showing that a reduced radiation dose treatment appears to be as effective as standard of care after three years. This treatment involves TORS (robotic surgery) in combination with 50 Gy (low dose) radiotherapy and no chemo. The idea behind this is to improve the quality of life by having less damage from the radiation while maintaining high survival benefits. 95% of the patients in the trial were alive and disease free three years after treatment. The trial is continuing.
From the story: “For intermediate-risk patients – those with uninvolved surgical margins, less than five involved nodes, and less than 1mm extranodal extension – postoperative radiation therapy at 50 Gy without chemotherapy appears sufficient."
Ferris, F.L. et al Phase II Randomized Trial of Transoral Surgery and Low-Dose Intensity Modulated Radiation Therapy in Resectable p16+ Locally Advanced Oropharynx Cancer: An ECOG-ACRIN Cancer Research Group Trial (E3311) DOI: 10.1200/JCO.21.01752 Journal of Clinical Oncology
——————————————————————————————————————————————
Here’s a nice synopsis of ongoing radiotherapy trials for patients with locally advanced HPV-positive head and neck cancers:
Transoral Robotic Surgery Followed by Adjuvant Radiotherapy
Definitive Radiotherapy With Chemotherapy Cetuximab and/or Immunotherapy
Personalized Chemoradiation Therapy Based on Hypoxia Imaging -
29) Are HPV Infections Associated With Skin Squamous Cell Carcinomas?
- Maybe, but only under particular circumstances. This has been looked at a number of times, but no definitive answer has emerged. The idea here is that strains of HPV that are found on skin and cause common warts, and are generally considered to be non-cancer forming, can help cause skin cancers under certain circumstances. These potential co-factors could include exposure to damaging UV radiation, or being immunocompromised.
If this hypothesis was true, then we might expect to find a lower incidence of SCC in people who have been immunized against cutaneous HPV strains. There have been three HPV vaccines on the market, Cervarix, Gardasil, and Gardasil 9. The latter two vaccines immunize against two wart causing strains of the virus, 6 and 11. This would suggest that those immunized with Gardasil or Gardasil 9 might have a lower incidence of skin SCC than those immunized with Cervarix.
See the following:
Potential Role of the HPV Vaccine in Preventing Non-Melanoma Skin Cancers
Wang et al. Role of human papillomavirus in cutaneous squamous cell carcinoma: A Meta-analysis. J Am Acad Dermatol. 2014 April ; 70(4): 621–629. doi:10.1016/j.jaad.2014.01.857. FREE download
Vinson and Rosa. HPV vaccination for prevention of skin cancer. Hum Vaccin Immunother. 2015 Feb; 11(2): 353–357. doi: 10.4161/21645515.2014.983858 FREE download
Are there some circumstances were HPV might contribute to skin squamous cell carcinoma?. Looks like the answer is yes. Skin cancer is generally caused by UV radiation from the sun, not the HPV virus. There are many different types of HPV, each tending to infect cells in a particular tissue and part of the body. The strains of HPV found mostly on the skin—beta-HPV—are considered innocuous viruses on your skin; they don't typically integrate into the DNA of skin cells and cause problems. This contrasts them with the alpha types of HPV, known to integrate into the DNA of mucous membrane cells and directly cause cancer of the genitals, anus, cervix, and head and neck.
The thinking about these beta HPV cancers changed when researchers at the NIH examined a 34-year-old woman who came in for evaluation and treatment of recurrent cSCC (cutaneous squamous cell carcinoma) on her forehead. "She had undergone multiple surgeries and a round of immunotherapy to try to remove or kill the tumor, but it repeatedly grew back. Her local doctors thought this was due to an inherited inability to repair DNA damaged by UV radiation plus an impairment in immune cells called T cells. The tumor was one of many progressively worsening HPV-related diseases the woman was experiencing.
Through a sophisticated genetic analysis, the NIH researchers discovered that a beta-HPV had integrated into the cellular DNA of the woman’s well-established tumor and was extensively producing viral proteins there. This contradicted the prevailing theory that beta-HPV only facilitates the establishment of cSCC without integrating into cellular DNA and plays no role in maintaining the cancer. Further genetic analysis of the woman’s cells showed they were fully capable of repairing DNA damage from UV radiation, suggesting the virus alone had caused cSCC.
To understand how beta-HPV could take the unusual steps of integrating into the woman’s skin-cell DNA and multiplying there unchecked, the investigators studied the woman’s inherited immune disorder. They found that her genetic mutations greatly hampered T cells from activating in response to skin-cell infection by beta-HPV. This suggested that the immune disorder itself was responsible for the woman’s worsening HPV-related diseases, including the beta-HPV cSCC on her forehead, and that treating this disorder might cure all of them."
The NIH investigators developed a personalized plan to give the woman a stem cell transplant to replace the defective T cells of her immune system with healthy ones. Afterward, all her HPV-related diseases including the recurrent, aggressive cSCC resolved and have not recurred during the more than three years since the transplant. This confirms that the woman’s inherited disorder had prevented her T cells from keeping beta-HPV in check, allowing the virus to directly cause and sustain cSCC.
The key feature here is that the woman had an immune disorder. Without this, she would NOT have developed this HPV skin cancer. More details here. -
30) Do Underserved People With Head and Neck Cancers Have Worse Outcomes?
- A recent study says yes, they do. The reasons are multi-factorial and complicated, and are often tied to an inability to attend follow up appointments follow diagnosis. Here’s a brief summary of the issues, “First, initiation of treatment beyond 60 days after diagnosis is associated with worse survival (adjusted hazard ratio, 1.69; 95% CI, 1.32-2.18) and a higher risk of recurrence (adjusted odds ratio, 1.77; 95% CI, 1.07-2.93) after adjustment for relevant covariates. Second, key variables are independently associated with delayed treatment initiation, including fragmentation of care between diagnosis and treatment facilities, African American race, and Medicaid insurance. Third, the most common reasons for delayed treatment are missed appointments, extensive pretreatment evaluation, and treatment refusal.”
Graboyes, E.M, and Hughes-Halbert. Delivering Timely Head and Neck Cancer Care to an Underserved Urban Population—Better Late Than Never, but Never Late Is Better. JAMA Otolaryngol Head Neck Surg. Published online September 12, 2019. doi:10.1001/jamaoto.2019.2432
—————————————————————————————————————————————————————————————————————
Here’s another paper that came to the same conclusion, showing that Black patients have worse overall survival than whites, even after controlling for age, sex, cancer stage, smoking, alcohol use, and individual-level household income, insurance, and education level. This is the first population-based study that confirms persistence of racial disparities in HPV-associated oropharyngeal squamous cell carcinoma after controlling for demographic, clinical, and individual-level socioeconomic factors.
Sheth, S. et al. Decreased overall survival in black patients with HPV-associated oropharyngeal cancer. American Journal of Otolaryngology Volume 42, Issue 1, January–February 2021, 102780 https://doi.org/10.1016/j.amjoto.2020.102780 FREE download.
—————————————————————————————————————————————————————————————————————
In another study of racial differences, researchers looked at age-adjusted incidence trends, late-stage diagnosis, survival, and cancer-specific mortality (CSM) among males diagnosed with HPV-related OPC. What did they find?
“Results: The majority of the 162,183 HPV-related OPCs were in non-Hispanic (NH) White males (84.2%), with 50% increase in late-stage cancer incidence among White males from 2005 to 2016. Despite having similar odds of late-stage diagnosis as White males, Hispanic and NH Black males had higher CSM [adjusted hazard ratios (aHR) 1.17; 95% confidence interval (CI): 1.08, 1.26, and aHR 1.79; 95% CI: 1.71, 1.88, respectively]. Adjusting for treatment attenuated, but did not eliminate, the higher mortality in Hispanic and Black males.
Conclusions: NH White males are disproportionately affected by late-stage HPV-related OPC, while Hispanic and NH Black males have higher CSM that was not explained by stage or treatment modality. Interventions to increase HPV vaccine uptake, early detection, and treatment of OPC in males are needed to decrease disparities in incidence and mortality.”
Villalona, S. et al Racial/ethnic disparities in HPV-related oropharyngeal cancer outcomes among males in the United States: a national cohort study. Annals of Cancer Epidemiology, 2022. FREE download.Lorem ipsum dolor sit amet, sapien platea morbi dolor lacus nunc, nunc ullamcorper. Felis aliquet egestas vitae, nibh ante quis quis dolor sed mauris. Erat lectus sem ut lobortis, adipiscing ligula eleifend, sodales fringilla mattis dui nullam. Ac massa aliquet. -
31) Are Female Prisoners at Greater Risk Of HPV Infection and Cervical Cancer?
- The short answer is yes. A total of 53,533 imprisoned women from 10 countries and 35 studies were included in a recent review. The prevalence of HPV among prisoners ranged from 10.5% to 55.4% with significant heterogeneity. The prevalence of CIN diagnosed by cytology in prisoners ranged from 0% to 22%. Ratios comparing the prevalence of CIN in imprisoned women to that in the community ranged from 1.13 to 5.46. Cancer prevalence estimates were at least 100 times higher than in populations participating in national screening programs in those same countries. The authors concluded that imprisoned women are at higher risk of cervical cancer than the general population. There is a high prevalence of HPV infection and precancerous lesions in this population. They recommend targeted programs for control of risk factors and the development of more effective cervical screening programs.
-
32) Are Oral Cancer Recurrences Often Found During Follow Up Appointments?
- The short answer is usually no. Very few recurrences are found via the patient visits; most recurrences are found when the patients notice symptoms and then contacts their doctors. As the report concluded, “Among patients with HPV-associated OPSCC, clinical surveillance is of limited utility. Nearly all clinically detected recurrences were elicited by patient symptoms that prompted earlier presentation to the clinician. Adherence to the current schedule does not appear to confer survival advantage, and locoregional recurrences are almost never detected beyond 2 years. These findings support reduction of post-treatment clinical surveillance in this population.”
Masroor, F. et al Association of NCCN-Recommended Posttreatment Surveillance With Outcomes in Patients With HPV-Associated Oropharyngeal Squamous Cell Carcinoma. JAMA Otolaryngol Head Neck Surg. 2019;145(10):903-908. doi:10.1001/jamaoto.2019.1934 Key Points -
33) Does Delaying Treatment Affect H&N Cancer Recurrence And Survival Rates?
- This was looked at via a retrospective study in an underserved group of nearly 1,000 patients at a single medical institution over a 14 year period. The bottom line: delaying time to treatment initiation (TTI) beyond 60 days was associated with decreased overall survival and increased HNSCC recurrence.
Predictors of delayed TTI included African American race/ethnicity, Medicaid insurance, body mass index less than 18.5, and initial diagnosis at a different institution.
Commonly identified individual reasons for treatment delay were missed appointments (21.2%), extensive pretreatment evaluation (21.2%), and treatment refusal (13.6%). The reasons for this are complex and are discussed in the freely available commentary listed below.
Liao, D.Z. Association of Delayed Time to Treatment Initiation With Overall Survival and Recurrence Among Patients With Head and Neck Squamous Cell Carcinoma in an Underserved Urban Population. JAMA Otolaryngol Head Neck Surg. 2019;145(11):1001-1009. doi:10.1001/jamaoto.2019.2414
This paper was accompanied by a well written editorial piece Delivering Timely Head and Neck Cancer Care to an Underserved Urban Population—Better Late Than Never, but Never Late Is Better. Graboyes, E.M, and Hughes-Halbert, C., JAMA Otolaryngol Head Neck Surg. 2019;145(11):1010-1011. doi:10.1001/jamaoto.2019.2432 (FREE DOWNLOAD) -
34) Are Anal Cancer Rates Increasing In the US, And For Which Groups?
- The short answer is yes. An analysis of US Cancer statistics from the period 2001-2016 showed that squamous cell cancer of the anus (SCCA), which is mostly caused by HPV, increased for several groups. SCCA incidence increased 2.7% per year with pronounced increases in age groups 50 years and older. Distant stage (i.e. metastasized) SCCA incidence tripled among men and women, and regional stage SCCA incidence nearly doubled in both sexes. Compared to adults born circa 1946, recent born Black men (born circa 1986) had nearly fivefold higher risk of SCCA and the risk doubled among White men and White women born after circa 1960. Anal cancer mortality rates increased 3.1% per year with statistically significant increases in age groups 50 years and older. Incidence-based mortality increased 1.9% annually with a notable rise in 60-69-year-old adults.
Ashish A Deshmukh, A.A. et al Recent trends in squamous cell carcinoma of the anus incidence and mortality in the United States, 2001-2015.
Journal of the National Cancer Institute, djz219, https://doi.org/10.1093/jnci/djz219
———————————————————————————————————————————————————————————————————————————————————————————
Note also that people with anal cancers that are HPV positive have better overall survival than those whose cancers are HPV negative. This mirrors the findings for oropharyngeal cancer.
Urbute, A. et al. Prognostic Significance of HPV DNA and p16INK4a in Anal Cancer: A Systematic Review and Meta-Analysis. Cancer Epidemiol Biomarkers Prev 2020 doi: 10.1158/1055-9965.EPI-19-1259 -
35) Does The Microbiome Play A Role In The Development Of HPV Cancers?
- The short answer appears to be yes, at least in the case of cervical cancer. The bacteria in the vagina/cervix can play a role in the immune response to HPV infections . This is not well understood yes, but it may be possible to alter the microbiome (essentially, the types of bacteria that live in the vagina/cervix) as a way to fight off HPV infections. Doing so in other locations (e.g. the oral cavity) may be more difficult to modulate.
To learn more, see Microbiome insights open new avenues to treat HPV as well as Sharifian, K. et al The interplay between human papillomavirus and vaginal microbiota in cervical cancer development. Virol J 20, 73 (2023). https://doi.org/10.1186/s12985-023-02037-8 -
36) Are HPV infections Associated With Cardiovascular Disease?
- Sadly, the answer may be yes. In addition to causing cancer, a meta-analysis being presented on March 31 at the American College of Cardiology’s (ACC's) Annual Scientific Session in Chicago suggests that HPV also poses a significant risk of cardiovascular disease.
For the University of Connecticut review, researchers analyzed 7 studies conducted from 2011 to 2024 that included the HPV status and cardiovascular outcomes of 249,366 patients over follow-up times of 3 to 17 years. Most were retrospective and longitudinal cohort studies, 3 each were from the United States and South Korea, and 1 each was from Brazil and Australia.
The researchers examined the relationship between HPV and cardiovascular disease, coronary artery disease, and high blood pressure in pooled study cohorts. Some analyses adjusted for potential confounding factors such as smoking and diabetes.
Relative to HPV-negative participants, HPV patients had a 40% higher risk of cardiovascular disease and twice the risk of coronary artery disease, but no increased rate of high blood pressure. After adjusting for factors such as sociodemographics, medical history, lifestyle, family history, and use of blood pressure–lowering drugs, HPV patients had a 33% higher risk of cardiovascular disease. "The biological mechanism has not been determined but is hypothesized to be related to chronic inflammation," lead author Stephen Akinfenwa, MD, of UConn, said in the ACC press release. "We would ultimately like to see if reducing HPV via vaccination could reduce cardiovascular risk."
Akinfenwa said clinicians should closely monitor HPV patients' hearts. "We always talk about cardiovascular risk factors like smoking, high blood pressure and so on, but we know that about 20% of cardiovascular disease cannot be explained by these conventional risk factors," he said.