http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#1
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#2
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#3
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#4
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#5
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#6
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#7
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#8
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#9
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#10
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#11
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#12
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/#13
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#1
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#2
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#3
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#4
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#5
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#6
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#7
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#8
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#9
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/#10
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#1
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#2
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#3
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#4
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#5
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#6
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#7
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#8
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#9
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#10
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#1
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#2
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#3
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#4
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#5
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#6
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#7
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#8
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#9
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#10
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#11
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#12
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#13
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#14
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#15
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#16
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/#17
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#1
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#2
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#3
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#4
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#5
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#6
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#7
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#8
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#9
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#10
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#11
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#12
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#13
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#14
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#15
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#16
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#17
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#18
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#19
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#20
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#21
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#22
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#23
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#24
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#25
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#26
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#27
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#28
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#29
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#30
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#31
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#32
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#33
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/#34
http://www.hpvcancerresources.org/HPVFAQ/#1
http://www.hpvcancerresources.org/HPVFAQ/#2
http://www.hpvcancerresources.org/HPVFAQ/#3
http://www.hpvcancerresources.org/HPVFAQ/#4
http://www.hpvcancerresources.org/HPVFAQ/#5
http://www.hpvcancerresources.org/HPVFAQ/#6
http://www.hpvcancerresources.org/HPVFAQ/#7
http://www.hpvcancerresources.org/HPVFAQ/#8
http://www.hpvcancerresources.org/HPVFAQ/#9
http://www.hpvcancerresources.org/HPVFAQ/#10
http://www.hpvcancerresources.org/HPVFAQ/#11
http://www.hpvcancerresources.org/HPVFAQ/#12
http://www.hpvcancerresources.org/HPVFAQ/#13
http://www.hpvcancerresources.org/HPVFAQ/#14
http://www.hpvcancerresources.org/HPVFAQ/#15
http://www.hpvcancerresources.org/HPVFAQ/#16
http://www.hpvcancerresources.org/HPVFAQ/#17
http://www.hpvcancerresources.org/HPVFAQ/#18
http://www.hpvcancerresources.org/HPVFAQ/#19
http://www.hpvcancerresources.org/HPVFAQ/#20
http://www.hpvcancerresources.org/HPVFAQ/#21
http://www.hpvcancerresources.org/HPVFAQ/#22
http://www.hpvcancerresources.org/HPVFAQ/#23
http://www.hpvcancerresources.org/HPVFAQ/#24
http://www.hpvcancerresources.org/HPVFAQ/#25
http://www.hpvcancerresources.org/HPVFAQ/#26
http://www.hpvcancerresources.org/HPVFAQ/#27
http://www.hpvcancerresources.org/HPVFAQ/#28
http://www.hpvcancerresources.org/HPVFAQ/#29
http://www.hpvcancerresources.org/HPVFAQ/#30
http://www.hpvcancerresources.org/HPVFAQ/#31
http://www.hpvcancerresources.org/HPVFAQ/#32
http://www.hpvcancerresources.org/HPVFAQ/#33
http://www.hpvcancerresources.org/HPVFAQ/#34
http://www.hpvcancerresources.org/HPVFAQ/#35
http://www.hpvcancerresources.org/HPVFAQ/#36
http://www.hpvcancerresources.org/HPVFAQ/#37
http://www.hpvcancerresources.org/HPVFAQ/#38
http://www.hpvcancerresources.org/HPVFAQ/#39
http://www.hpvcancerresources.org/HPVvaccineFAQ/#1
http://www.hpvcancerresources.org/HPVvaccineFAQ/#2
http://www.hpvcancerresources.org/HPVvaccineFAQ/#3
http://www.hpvcancerresources.org/HPVvaccineFAQ/#4
http://www.hpvcancerresources.org/HPVvaccineFAQ/#5
http://www.hpvcancerresources.org/HPVvaccineFAQ/#6
http://www.hpvcancerresources.org/HPVvaccineFAQ/#7
http://www.hpvcancerresources.org/HPVvaccineFAQ/#8
http://www.hpvcancerresources.org/HPVvaccineFAQ/#9
http://www.hpvcancerresources.org/HPVvaccineFAQ/#10
http://www.hpvcancerresources.org/HPVvaccineFAQ/#11
http://www.hpvcancerresources.org/HPVvaccineFAQ/#12
http://www.hpvcancerresources.org/HPVvaccineFAQ/#13
http://www.hpvcancerresources.org/HPVvaccineFAQ/#14
http://www.hpvcancerresources.org/HPVvaccineFAQ/#15
http://www.hpvcancerresources.org/HPVvaccineFAQ/#16
http://www.hpvcancerresources.org/HPVvaccineFAQ/#17
http://www.hpvcancerresources.org/HPVvaccineFAQ/#18
http://www.hpvcancerresources.org/HPVvaccineFAQ/#19
http://www.hpvcancerresources.org/HPVvaccineFAQ/#20
http://www.hpvcancerresources.org/HPVvaccineFAQ/#21
http://www.hpvcancerresources.org/HPVvaccineFAQ/#22
http://www.hpvcancerresources.org/HPVvaccineFAQ/#23
http://www.hpvcancerresources.org/HPVvaccineFAQ/#24
http://www.hpvcancerresources.org/HPVvaccineFAQ/#25
http://www.hpvcancerresources.org/HPVvaccineFAQ/#26
http://www.hpvcancerresources.org/HPVvaccineFAQ/#27
http://www.hpvcancerresources.org/HPVvaccineFAQ/#28
http://www.hpvcancerresources.org/HPVvaccineFAQ/#29
http://www.hpvcancerresources.org/HPVvaccineFAQ/#30
http://www.hpvcancerresources.org/HPVvaccineFAQ/#31
http://www.hpvcancerresources.org/HPVvaccineFAQ/#32
http://www.hpvcancerresources.org/HPVvaccineFAQ/#33
http://www.hpvcancerresources.org/HPVvaccineFAQ/#34
http://www.hpvcancerresources.org/HPVvaccineFAQ/#35
http://www.hpvcancerresources.org/HPVvaccineFAQ/#36
http://www.hpvcancerresources.org/HPVvaccineFAQ/#37
http://www.hpvcancerresources.org/HPVvaccineFAQ/#38
http://www.hpvcancerresources.org/HPVvaccineFAQ/#39
http://www.hpvcancerresources.org/HPVvaccineFAQ/#40
http://www.hpvcancerresources.org/HPVvaccineFAQ/#41
http://www.hpvcancerresources.org/HPVvaccineFAQ/#42
http://www.hpvcancerresources.org/HPVvaccineFAQ/#43
http://www.hpvcancerresources.org/HPVvaccineFAQ/#44
http://www.hpvcancerresources.org/HPVvaccineFAQ/#45
http://www.hpvcancerresources.org/HPVvaccineFAQ/#46
http://www.hpvcancerresources.org/HPVFAQ/#40
http://www.hpvcancerresources.org/HPVFAQ/#41
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/#11
http://www.hpvcancerresources.org/patientinfo/hottopics/#1
http://www.hpvcancerresources.org/patientinfo/hottopics/#2
http://www.hpvcancerresources.org/patientinfo/hottopics/#3
http://www.hpvcancerresources.org/patientinfo/hottopics/#4
http://www.hpvcancerresources.org/patientinfo/hottopics/#5
http://www.hpvcancerresources.org/patientinfo/hottopics/#6
http://www.hpvcancerresources.org/patientinfo/hottopics/#7
http://www.hpvcancerresources.org/patientinfo/hottopics/#8
http://www.hpvcancerresources.org/HPVvaccineFAQ/HPVvaccinemisinformation/index.html
http://www.hpvcancerresources.org/patientinfo/supportadvocacygroups/index.html
http://www.hpvcancerresources.org/patientinfo/patientcaregiversresources/index.html
http://www.hpvcancerresources.org/HPVFAQ/HPVcancerscreening/index.html
http://www.hpvcancerresources.org/HPVFAQ/HPVepidemiology/index.html
http://www.hpvcancerresources.org/HPVvaccineFAQ/index.html
http://www.hpvcancerresources.org/HPVFAQ/index.html
http://www.hpvcancerresources.org/patientinfo/hottopics/index.html

The HPV Vaccine is Both Safe and Effective - FAQ
The HPV vaccine has been a tremendous advance in human health care.
We have solid data that shows the HPV vaccine:
Blocks infection with the human papilloma virus (HPV).
Prevents the occurrence of genital and anal warts.
Prevents cervical precancers, as well as cervical cancers.
Prevents anal high-grade squamous intraepithelial lesions (HSIL) and anal cancers.
Prevents oral HPV infections.
Reduces the occurrence of head and neck cancers in males.
Significantly reduces serious pregnancy-related complications including pre-eclampsia.
Details below, and in FAQ#3
What most people want to know are two things: is the HPV vaccine safe, and is it effective?
The answer to both questions is a clear YES!
In 2025, two Cochrane Library reviews were published on the safety and efficacy of the HPV vaccine. Cochrane reviews are considered the most in-depth and reliable scientific analysis studies. What did they show?
Review 1: Trial‑based network meta‑analysis of different HPV vaccines and schedules.
Title: “Human papillomavirus (HPV) vaccination for the prevention of cervical cancer and other HPV‑related diseases: a network meta‑analysis.”
Scope: Compares WHO‑prequalified vaccines (bivalent, quadrivalent, 9‑valent) and dose schedules in females and males using randomized controlled trials, focusing on CIN2+, CIN3+, anogenital warts and safety.
Key findings: HPV vaccination reduces high‑grade cervical precancer (CIN2+) and anogenital warts, with no cancer endpoints yet and no safety signals identified.
Reviews 2: Population‑level program effects review
Title: “Effects of human papillomavirus (HPV) vaccination programmes on community rates of HPV‑related disease and harms from vaccination.”
Scope: Synthesizes observational and ecological data from multiple countries, assessing incidence of high‑grade CIN, cervical cancer, other HPV‑related disease, and serious adverse events after programme rollout.
Key findings: Vaccination programs substantially reduce high‑grade CIN and cervical cancer when girls are vaccinated in early adolescence, with no evidence of increased serious adverse events such as Guillain‑Barré syndrome
In Jan. 2026, the Vaccine Integrity Project (established in 2025) announced that it was going to conduct its own independent review of the HPV vaccine. This was in response to Robert F. Kennedy Jr.'s criticisms of the vaccine, and who has called it "the most dangerous vaccine ever created," which does not match the actual data at all.
There’s a lot of information in the FAQs below on the HPV vaccine. It’s been approved in the US by the FDA for the prevention of cervical, anal, and certain head and neck cancers. Data obtained from hundreds of millions of vaccine doses given all around the world show that the vaccine is quite safe; details can be found in FAQ2. As for effectiveness, data was recently published showing that the HPV vaccine led to an 87% reduction in cervical cancer rates in England for girls who were given the vaccine when there were 12 or 13 years old. This expands on many previous studies showing the vaccine worked very well at blocking infection by HPV, reducing the occurrence of genital warts that are also caused by the virus, and led to a large decrease in cervical pre-cancers as well. Details can be found in FAQ#3.
Since the virus is thought to cause six different types of cancer, we can eventually expect to see reductions in those other types over time. Collecting that data is going to take a long while because the average time following infection for the development of these other types of cancer often takes decades. For example, HPV-caused oropharyngeal cancers (those at the back of the mouth and throat) are most commonly diagnosed when men and women are in their 60’s. We do know that the vaccine is effective is blocking infection with the virus in both men and women, so it’s just a matter of time until those reductions in cancer rates can be measured.
in 2022 Wang et al published Real-world impact and effectiveness of the quadrivalent HPV vaccine: an updated systematic literature review. EXPERT REVIEW OF VACCINES 2022, VOL. 21, NO. 12, 1799–1817 https://doi.org/10.1080/14760584.2022.2129615
Essentially, this article looked at all of the data that has been accumulated to date in 138 peer-reviewed publications reporting HPV vaccine impact or effectiveness. The overall conclusion: “HPV vaccination programs continue to support a marked reduction in new HPV infections and corresponding disease outcomes.” Many of these papers are discussed in the sections below.
Note that this study was funded by Merck, which makes the primary HPV vaccine in use today.
In 2024 an abstract was presented at the American Society of Clinical Oncology meeting with real world data on the effectiveness of the original HPV vaccine. What did that data show?
"Results from a new research study show that the human papillomavirus (HPV) vaccine lowers the chances of developing cancer caused by HPV, including head and neck cancer in men and boys and cervical cancer in women and girls.
The most common cancer caused by HPV worldwide is cervical cancer, although in the US it is oropharyngeal cancer.. Since the approval of the HPV vaccine in the United States in 2006, many studies have shown that the HPV vaccine reduces the risk of cervical cancer. However, other cancers can be caused by HPV, including head and neck cancer, anal cancer, penile cancer, vulvar cancer, and vaginal cancer. This study compared the risk of developing all HPV-related cancers in people who received the HPV vaccine with those who did not.
This study is a retrospective analysis. This type of research compares 2 or more groups of people by looking at data that has already been collected in the past. This study looked at data from 3,413,07 people ages 9 to 39 years old who had a medical visit where any vaccine was given between January 1, 2010, and December 31, 2023. The study population was divided into 2 groups: people who had received the HPV vaccine at least 5 years earlier (1,706,539 people) and those who had not received the HPV vaccine (1,706,538 people). Their average age was 21 years, 56% were women, and 53% were White, 21% were Black, 5% were Asian, 0.4% were American Indian or Alaskan Native, 0.4% were Native Hawaiian, and 21% were of other or unknown race.
Men and boys vaccinated for HPV had a lower risk of developing all HPV-related cancers compared to unvaccinated men and boys. In this group, there were 3.4 cases of HPV-related cancer for every 100,000 vaccinated patients compared to 7.5 cases of HPV-related cancer for every 100,000 unvaccinated patients. HPV vaccination also lowered the risk of developing head and neck cancers among men and boys. There were 2.8 cases of head and neck cancer for every 100,000 vaccinated patients, compared to 6.3 cases for every 100,000 unvaccinated patients.
Women and girls vaccinated for HPV also had a lower risk of developing all HPV-related cancers. In this group, there were 11.5 cases of HPV-related cancer for every 100,000 vaccinated patients, compared to 15.8 cases for every 100,000 unvaccinated patients. Women and girls who had received HPV vaccination also had a lower risk of developing cervical cancer. There were 7.4 cases of cervical cancer for every 100,000 vaccinated patients, compared to 10.4 cases for every 100,000 unvaccinated patients. Vaccinated women who had never had abnormal findings during a Pap test were also less likely to develop precancerous dysplasia of the cervix and undergo invasive procedures. Vaccinated women did not have a significantly lower risk of developing head and neck cancer or vaginal cancer when compared to those who did not receive the vaccine.
Because many HPV-related cancers are more common in older adults, research will continue to study outcomes in people older than 39 years of age.
What does this mean for patients? The HPV vaccine lowers the risk of developing HPV-related cancers in men and women, especially head and neck cancer in men and cervical cancer in women."
Here's another way of looking at the data from medical reporter Matthew Herper: "the data being presented at ASCO are based on the rates of HPV in a giant database of electronic health records from 90 million patients collected by TriNetX, a private company in the business of using such data to conduct observational studies. The researchers were able to compare roughly 1.7 million patients vaccinated for HPV with roughly the same number of age-matched control patients with no prior HPV vaccination. A total of 56% were female, 53% were white, 21% were Black/African American, with a mix of people of other backgrounds represented.
There are problems with this setup that actually make it tougher for the vaccine. For instance, some patients who had cervical lesions were known to get the vaccine after the lesions had shown up, and people might be getting the vaccine after they had already been infected with HPV, which takes many, many years to cause cancer. It’s also possible that some people who were included in the control group somehow got the vaccine and it wasn’t recorded, which would make the vaccine appear less effective.
Still, the results were dramatic. Vaccinated males had 3.4 cases of HPV-linked cancer per 100,000 patients compared to 7.5 per 100,000 unvaccinated patients. Vaccinated females had 11.5 cases per 100,000 patients compared to 15.8 per 100,000 unvaccinated patients."
———————————————————————————————————————————————————————————————————————
In Dec. 2025 new data came out indicating that the HPV vaccine was also effective at reducing the incidence of vulvar and vaginal pre-cancers. Researchers analyzed the medical records of 778,943 women, 32.9% of whom received at least one dose of the HPV vaccine (this was the older, quadrivalent vaccine). Median follow-up times were 17 years for unvaccinated women, 12.2 years for those vaccinated between the ages of 10 and 16, and 10.8 years for those vaccinated at 17 years or older.
The researchers identified 98 cases of high-grade vulvovaginal (either vulvar or vaginal pre-cancers) lesions among vaccinated women and 547 cases in the unvaccinated women. The vaccinated group of women included those who received as few as one of the recommended three doses of the quadrivalent vaccine.
In summary:
Women vaccinated against HPV had a 37% lower risk of developing high-grade vulvovaginal pre-cancerous lesions compared with unvaccinated women.
The risk reduction increased to 55% for those vaccinated between the ages of 10 and 16, emphasizing the benefits of early vaccination against HPV.
These results support other studies that show a lower risk of vulvovaginal pre-cancers and cancers among vaccinated women.
This new study adds to the body of evidence that the HPV vaccine not only prevents cervical cancers, but it also reduces the risk of high-grade vulvovaginal lesions, which can lead to vulvar and vaginal cancer.
As the initial cohort of men and women who received the HPV vaccine grows older, there are likely to be more studies that will provide evidence that the vaccine prevents other HPV-related cancers.
-
1) Is There A Safe And Effective Vaccine Against HPV?
- According to the CDC, An Estimated 92% of Cancers Caused by HPV Could be Prevented by the HPV Vaccine
This vaccine is both safe and effective, and has been extensively tested.
It is currently approved by the US FDA to prevent cervical cancer, anal cancer, and head and neck cancers, along with genital warts caused by HPV.
According to the National Cancer Institute, “The Food and Drug Administration (FDA) has approved three vaccines that prevent infection with disease-causing HPV types: Gardasil®, Gardasil® 9, and Cervarix®. All three vaccines prevent infection with HPV types 16 and 18, two high-risk HPVs that cause about 70% of cervical cancers and an even higher percentage of some of the other HPV-caused cancers. Gardasil also prevents infection with HPV types 6 and 11, which cause 90% of genital warts. Gardasil 9 prevents infection with the same four HPV types plus five additional cancer-causing types (31, 33, 45, 52, and 58).
As of May 2017, Gardasil 9 is the only FDA approved HPV vaccine available for use in the United States. Cervarix and Gardasil are still used in other countries.”
Historically:
Merck’s Gardasil vaccine was FDA approved in June, 2006; it was sold in Europe under the trade name Silgard. Initially it was only approved for girls; the FDA added treatment for boys in October 2009. This initial vaccine was targeted at four strains of the virus. The current vaccine, Gardasil 9, targets nine different strains of the virus.
GSK’s Cervarix vaccine was FDA approved in Oct. 2009; Cervarix was withdrawn from the U.S. market in Oct. 2016.
Merck’s Gardsil 9 vaccine won FDA approval in Dec. 2014. It replaced the original Gardasil vaccine.
Merck announced in 2024 that they were looking into expanding the strains covered by their vaccine to cover additional viral subtypes beyond the nine in Gardasil 9. They are also initiating trials of a single dose vaccine to hopefully replace the current three dose regimen (if given when girls or boys are 15 years or older).
China launched their own nine-valent HPV vaccine Cecolin for their domestic market in June 2025. This follows on the May 2020 launch of a bivalent HPV vaccine by the same name that covered HPV strains 16 and 18. For additional details, see FAQ 29 below.
India is launching their own HPV vaccine,Cervavac, starting in 2022, make by the Serum Institute of India. The vaccine will be administered via injection in two doses among 9-14 year olds and in three doses for those between 15 and 26. It is a quadravalent vaccine against strains 6, 11, 16, and 18 (the same strains covered by Merck’s original Gardasil vaccine).
Bangladesh has launched its own bivalent vaccine against strains 16 and 18 know as Papilovax in 2022. It’s made by Incepta Vaccine Ltd.
According to the CDC, the Gardasil 9 HPV vaccine is recommended for all boys and girls ages 11-12; the vaccine can be given as early as age 9. Gardasil 9 is currently given on a two dose immunization schedule for those who are 14 years old or younger. Those who are 15 years old or older get 3 doses of the vaccine. HPV vaccination was recommended through age 26 for women, and through age 21 for men, if they did not get vaccinated when they were younger. This changed in Oct. 2018 when the vaccine was approved to be given to men and women in the 27-45 age range as well (this includes men in the 21-26 year range). Even more recently (June 2019), the US Advisory Committee on Immunization Practices (ACIP) decided in a unanimous vote to recommend catch-up vaccinations with the HPV vaccine for young women and men up to the age of 26 who have not previously received three doses of the vaccine. Although the Food and Drug Administration recently extended the age indication for the vaccine to allow people aged 27 to 45 to be vaccinated, ACIP did NOT recommend all people in that age group get the three-dose vaccine. Instead, the committee voted to leave the choice to patients and their doctors. ACIP recommended that the vaccine be given between the ages of 11 and 12 (though it can be started as early as 9 years old) in both girls and boys. Catch-up vaccination programs were recommended for young women up to the age of 26 who were not vaccinated earlier. The catch-up program for young men was to the age of 21; the vaccine was also recommended for males between the ages of 21 and 26 who have sex with men and those who are immunocompromised.
Note: A new science article in March 2021 suggests that giving the HPV vaccine to men or women in the 26 to 45 year old range (where it currently does have FDA approval) is not cost effective.
This doesn't mean that there aren't benefits in some individual cases, only that across the entire population in the US, the money spent vaccinating will be greater than the costs (financial; not emotional or physical) saved by doing so. It's a complex subject, and you can read more here. Unclear if this will result in any changes in the FDA approval or other recommendations. FYI.
https://www.eurekalert.org/pub_releases/2021-03/p-hvm030421.php
Here’s the actual paper: Kim, J.J. et al Human papillomavirus vaccination for adults aged 30 to 45 years in the United States: A cost-effectiveness analysis. PLOS Medicine https://doi.org/10.1371/journal.pmed.1003534
The American Cancer Society updated it’s guidance on the vaccine in July 2020: it’s encouraging health care providers to start offering the cancer-preventing vaccine sooner, at ages 9-10.
On the issue of whether to recommend catch-up vaccination for people aged 27 to 45, the committee voted 10-to-4 to leave that decision to patients and their doctors. There would be some people in that age group that would benefit from getting vaccinated, a number of the members noted. A working group that advised the committee noted that recommending vaccination of all adults 27 to 45 would NOT be a reasonable use of resources.
HPV vaccination is also recommended for the following people through age 26, if they did not get vaccinated when they were younger:
Young men who have sex with men or are bisexual
Young adults who are transgender
Young adults with weakened immune systems
According to Merck, the vaccines manufacturer:
“GARDASIL®9 (Human Papillomavirus 9-valent Vaccine, Recombinant) helps protect girls and women ages 9 to 26 against cervical, vaginal, vulvar, and anal cancers and genital warts caused by 9 types of HPV. GARDASIL 9 helps protect boys and men ages 9 to 26 against anal cancer and genital warts caused by those same HPV types.
GARDASIL 9 may not fully protect everyone, nor will it protect against diseases caused by other HPV types or against diseases not caused by HPV.
GARDASIL 9 does not prevent all types of cervical cancer, so it’s important for women to continue routine cervical cancer screenings. GARDASIL 9 does not treat cancer or genital warts.”
Merck has created an HPV vaccine website in the US as well as one in the UK called HPVwise, with a limited set of FAQ
None of the vaccines contained live or attenuated virus. All are made against proteins that make up the structure of the virus (specifically, the L1 major capsid protein). As a result, you cannot get infected with HPV by the vaccine.
Currently available HPV vaccines do NOT contain Thiomersal (an authorized and harmless preservative used in some other vaccines), nor any other form of mercury.
The Kaiser Family Health Foundation has also produced a useful fact sheet about the HPV vaccine.
The National Foundation for Infectious Diseases has put forth a Call to Action for HPV Vaccination as a Public Health Priority
Check out the videos that are part of this archive of a 2017 conference Building Trust, Managing Risk:
Vaccine Confidence and Human Papillomavirus Vaccination. This was put on by the Vaccine Confidence Project, a London based group that works to restore confidence in and to fight misinformation about vaccines. Check out this free paper by Heidi Larson published in Nature The biggest pandemic risk? Viral misinformation Nature 562, 309 (2018) doi: 10.1038/d41586-018-07034-4
The extra cost of vaccinating men from 21 to 45 and women from 26 to 45 was estimated to a cost effective strategy. Source: Laprise, J.-F. et al Effectiveness and Cost-Effectiveness of Human Papillomavirus Vaccination Through Age 45 Years in the United States. Ann Intern Med. 2020;172(1):22-29. DOI: 10.7326/M19-1182Can We Switch Over to a One-Shot HPV Vaccine Protocol?
The answer to this question is a clear YES, but there are some important caveats. A large-scale randomized controlled trial from Costa Rica found that one dose of either a bivalent (two-strain) or nonavalent (nine-strain) human papillomavirus (HPV) vaccine provides the same protection against infection with the HPV16 or HPV18 types as the more common two-dose series, offering a potentially transformative tool for global cervical cancer prevention. This is important because HPV types 16 and 18 cause more than 77% of cervical cancers worldwide.
The study, Noninferiority of One HPV Vaccine Dose to Two Doses, published in The New England Journal of Medicine (NEJM) in December 2025, enrolled 20,330 girls ages 12 to 16 years old and followed up with them for five years. The rate difference between one and two doses of the bivalent vaccine was −0.13 infections per 100 participants, and the difference between one and two doses of the nonavalent vaccine was 0.21 infections per 100 participants. In all four trial groups, the vaccine was 97% effective, and protection did not wane during the follow-up period. The trial didn’t find any safety concerns in keeping with previous research. The safety profiles of HPV vaccines have been evaluated extensively in hundreds of millions of people and it has been shown to be safe and effective.
These results will be helpful in the US (where it is estimated about 77% of girls have gotten at least one shot of the current vaccine) and it has reduced the incidence of cervical pre-cancers by about 80%. In Scotland and Australia the vaccine is getting close to eliminating cervical cancer entirely. Having said that, the greatest value of the vaccine will be found outside of the US in less developed regions, where HPV infections can be a death sentence. The need for one shot, and not two, could facilitate getting the vaccine to the three-quarters of children globally who should receive the vaccines but don’t. The shots prevent cervical cancer as well as anal, penile, and some head-and-neck cancers. Worldwide, 350,000 women die from cervical cancer, the most common HPV cancer. These women haven't had access to the vaccine. They don't have access to yearly Pap smears or HPV testing.
Single-dose vaccination would help low-, middle- and high-income countries across the world overcome the financial and logistical challenges of getting people to return for multiple doses. It would also strengthen WHO’s cervical cancer–elimination strategy, which calls for 90% of girls to be fully vaccinated by age 15, 70% of adult women to be screened in their lifetime, and 90% of women with cervical cancer to receive appropriate treatment.
More details can be found here: One Dose of HPV Vaccine Noninferior to Two, Data Show
As a result of these studies, the CDC changed its recommendations in Jan. 2026 to a one shot HPV vaccine protocol. This follows the WHO shift to a one shot HPV vaccine protocol in 2022.
You can also get a feel for how this change can affect worldwide HPV vaccination rates in this story from STAT.
Why might it be a problem to switch from two shots to one?
There are some people who are uncomfortable with making this switch, since the long term consequences (i.e. how long the vaccine is effective for) are still unknown for the one shot protocol.
The key issue is that all of the data on going from two shots to one was in girls, and the cancer studied was always cervical cancer.
Here's what we don't know:
1) will boys do equally well with getting one shot vs getting two shots of the HPV vaccine? We don't know if their immune responses will be as robust as girls.
2) And while switching over to one shot clearly worked to reduce cervical pre-cancers and cancers in girls, we don't know if one shot will prevent HPV-caused oropharyngeal, anal, and/or penile cancers in men. It's reasonable to assume that it can do this, but there is no hard data to base that decision on.
Below are reports of earlier studies that also showed that switching to a one shot protocol can be effective against HPV.
—————————————————————————————————————————————————————————————————————————
In England they just announced that they were going to switch over to a one-shot protocol for both girls and boys in Sept. 2023 following the advice from the Joint Committee on Vaccination and Immunisation (JCVI) and World Health Organization scientists. The HPV vaccine program has been offered to children in school at the age of 12 to 13 as a two shot series and is used to prevent a range of cancers.
In July 2024, Canada's National Advisory Committee on Immunization began recommending one dose of HPV vaccine for children and youth between nine and 20 years old. It's maintaining its two-dose recommendation for people who are 21 to 26 years old.
The rest of the world may soon follow suit. The WHO Strategic Advisory Group of Experts on Immunization (SAGE) met in April 2022 and evaluated the evidence that has been emerging over past years that single-dose schedules provide comparable efficacy to the two or three-dose regimens.
SAGE’s review concluded that a single-dose Human Papillomavirus (HPV) vaccine delivers solid protection against HPV, the virus that causes cervical cancer, that is comparable to 2-dose schedules. This could be a game-changer for the prevention of the disease. Switching to a single dose means this life saving vaccine is more likely to reach more girls around the world.
According to PATH, “the Single-Dose HPV Vaccine Evaluation Consortium, coordinated by PATH, has gathered and evaluated data from clinical trials, observational studies, and modeling analyses regarding the value of a single-dose HPV vaccination schedule. The Consortium collated, synthesized, and evaluated evidence that contributed to WHO’s decision in 2022 to endorse a single-dose HPV vaccine schedule for the primary target age group (9–14 years old).”
A single-dose schedule can expand coverage, reaching more girls and preventing more cases of cervical cancer. While the Consortium continues to disseminate evidence and evaluate ongoing and additional clinical studies, the WHO endorsement provides reassurance that administration of a single dose will have a positive public health benefit while alleviating financial and logistical barriers.”
To expand access to HPV vaccines, the World Health Organization (WHO) announced that a fourth WHO-prequalified vaccine, Cecolin®, has been confirmed for use in a single-dose schedule in October 2024. A growing number of HPV vaccine products initially prequalified for use in a 2-dose schedule can now be used in a single-dose schedule. “Unlike most other cancers, we can eliminate cervical cancer, along with its painful inequities,” said Dr. Tedros Adhanom Ghebreyesus, WHO Director-General, in a press release on October 4, 2024.
“By adding another option for a one-dose HPV vaccination schedule, we have taken another step closer to consigning cervical cancer to history.”
The WHO also confirmed an additional HPV vaccine, Walrinvax®, is now the fifth product available on the global market. Walrinvax® is prequalified with a two-dose schedule. Further data will be needed to assess if this vaccine can be recommended for single-dose schedules in the future, says the WHO.
This analysis follows up on earlier data that suggested that suggested it might be possible to move to a one-injection vaccination routine in the future, rather than the current two or three vaccinations. “Julia Brotherton at the VCS Foundation in Australia and her colleagues analyzed cervical screening data from a quarter of a million Australian women who were eligible for the vaccination. During the study, sexually active women were encouraged to have a Pap smear test every two years to screen for cellular changes on the cervix that might be a sign of cancer. Analyzing registers of HPV vaccinations and cervical cancer cases, the team found that women who had received three doses of the vaccine were 41 per cent less likely to have these cellular changes – known as precancerous lesions – than unvaccinated women. Women who had been given one or two doses of the vaccine were, respectively, 35 and 39 per cent less likely than unvaccinated women to have these lesions. This suggests that even one dose of the vaccine can be enough to help lower the incidence of cervical cancer. Administering a one-dose vaccination campaign would be cheaper and easier to administer than a multi-dose program.”
The finding could be particularly useful in developing nations, which have the highest burden of cervical cancer but the least access to vaccines. It would mean a greater supply of vaccine would be available, and reduces worries about a shortage of the HPV vaccine.
Brotherton, J. et al Papillomavirus Research, DOI: 10.1016/j.pvr.2019.100177. Also see Brotherton, J.M. and Sundstroml More evidence suggesting that 1‐dose human papillomavirus vaccination may be effective. Cancer Feb. 2020. https://doi.org/10.1002/cncr.32696
A second study compared the efficacy of single dose, two doses, and three doses of the HPV vaccine in preventing HPV infection after ten years in adolescent girls age 10-18. Whether or not the girls were given one, two, or three shots of vaccine, the vaccine had at least 93% efficacy in preventing infections with the two most prevalent cancer causing strains of HPV, 16 and 18.
Basu, P. et al. Vaccine efficacy against persistent human papillomavirus (HPV) 16/18 infection at 10 years after one, two, and three doses of quadrivalent HPV vaccine in girls in India: a multicentre, prospective, cohort study. The Lancet Oncology. Published:October 08, 2021DOI: https://doi.org/10.1016/S1470-2045(21)00453-8. FREE Download.
A recent study in the US looked at giving 9-11 year old girls and boys a single shot of the HPV vaccine (it's difficult to get 2 or 3 vaccines into adolescents who don't have visits with their pediatricians nearly as often). Researchers enrolled the kids to receive the nonavalent HPV vaccine at intervals of 0, 24, and 30 months. Blood samples for antibodies to HPV-16 and HPV-18 (the two most carcinogenic strains) were obtained at the start and then every 6 months up to 30 months after the first vaccine dose. The authors found that antibody responses rose after the initial dose and remained stable through 24 months, and then the 24 month vaccine provided a booster response.
Zeng, Yi et al HPV 16/18 Antibody Responses After a Single Dose of Nonavalent HPV Vaccine. Pediatrics June 15, 2023. (10.1542/peds.2022-060301).
————————————————————————————————————————————
A recent study out of Kenya showed that a single dose vaccination protocol provided strong protection over a three year period. It should be noted that women who are HIV+ should get two doses of the HPV vaccine because they make a lesser immune response to the vaccine.
Here's the reference: Barnabas, R.V. et al Durability of single-dose HPV vaccination in young Kenyan women: randomized controlled trial 3-year results. Nat Med. 2023 Dec;29(12):3224-3232. doi: 10.1038/s41591-023-02658-0. Epub 2023 Dec 4. PMID: 38049621; PMCID: PMC10719107 FREE Download
————————————————————————————————————————————
Similar results have been published in a study of American women. According the the author’s discussion, “Our study suggests that US women who received 1 dose of the HPV vaccine may have gained similar protection against vaccine-type infections compared with those who received additional doses. These findings support previous observational studies and post hoc analyses of vaccine trials that demonstrated comparable effectiveness of 1 dose to 2 or 3 doses.”
Sonawane, K. et al. Prevalence of Human Papillomavirus Infection by Number of Vaccine Doses Among US Women. JAMA Netw Open. 2019;2(12):e1918571. doi:10.1001/jamanetworkopen.2019.18571 FREE Download.
————————————————————————————————————————————
In a separate analysis, researchers “examined information on females aged 9 to 26 years who were unvaccinated or who received one or more HPV vaccine doses between January 2006 and June 2015.
The analysis included 133,082 females (66,541 vaccinated and 66,541 unvaccinated). For females ages 15 to 19 years, those who received one, two, or three doses of the HPV vaccine had lower rates of preinvasive cervical disease than adolescents who were unvaccinated. Within five years, 2.65 percent of unvaccinated teens aged 15 to 19 years developed preinvasive cervical disease, compared with 1.62 percent, 1.99 percent, and 1.86 percent in the one-, two- and three-dose groups, respectively. The risk of pre-invasive cervical disease was 36 percent, 28 percent, and 34 percent lower for adolescents who received one, two, and three doses, respectively, compared with adolescents who were unvaccinated.
For the youngest (less than 15 years old) and oldest age groups (20 years and older), the investigators did not find significant differences among the vaccinated groups in terms of risk for preinvasive cervical disease.”
“This study shows the impact of vaccinating at younger ages and its lasting long-term protection against cervical cancer,” said Dr. Rodriguez. “It is important to educate parents about the need to vaccinate their children.”
Rodriguez, et al. (2020) Comparison of the long-term impact and clinical outcomes of fewer doses versus standard doses of human papillomavirus vaccine in the United States: a database study. CANCER. DOI: 10.1002/cncr.32700
Bottom line: A one vaccine protocol, if implemented, means that vaccination will be cheaper for both individuals and countries, and that supplies of the vaccine will allow for more people to be vaccinated.
————————————————————————————————————————————
In a 2021 study reported at the 34th International Papillomavirus Conference in Toronto, a randomized controlled trial of 2,275 women in Kenya showed that a single dose of the human papillomavirus (HPV) vaccine was highly effective. The current standard for women is a three-dose regimen. Currently, just 15% of women are vaccinated against HPV, according to an analysis published in March in Preventive Medicine.
In the trial, women 15 to 20 years old were randomly assigned a therapy and followed from December 2018 to June 2021:
760 received a bivalent vaccine that covered two strains of HPV (16/18), which represent 70% of cases;
758 received a nonavalent vaccine that covered seven strains of HPV (16/18/31/33/45/52/58), which represent 90% of cases;
757 received a vaccine that protects against meningococcal meningitis.
After 18 months, the bivalent vaccine was 97.5% effective against HPV 16/18 and the nonavalent vaccine was 97.5% effective against HPV 16/18. The nonavalent vaccine was 89% effective against HPV 16/18/31/33/45/52/58. Even if women tested positive for one strain of HPV, the vaccine protected them from other strains of the virus.Does It Matter At What Age the HPV Vaccine Is Given At?
The short answer is yes. Giving the shot before sexual debut turns out to be very important in providing the best protection. Why? Two reasons. The immune response is stronger at that age, and giving the vaccine after sexual debut, when the person may have already been infected with HPV, will be of much less value.
Details can be found here, and the full details are in this paper:
Egemen, D.; Katki, H.; and Chaturvedi, A.K. Variation in Human Papillomavirus Vaccination Effectiveness in the US by Age at Vaccination. JAMA Netw Open. 2022;5(10):e2238041. doi:10.1001/jamanetworkopen.2022.38041
Here are the results:
“Among the 4727 female individuals (mean [SD] age, 17.9 [0.2] years) ever eligible for vaccination, cervical HPV-16/18 prevalence decreased from 6% (95% CI, 4%-7%) in the unvaccinated group to 3% (95% CI, 1%-6%) in the postdebut group and less than 1% (95% CI, <1%-1%) in the predebut group (Figure). HPV-16/18 prevalence was 89% (P < .001) lower in the predebut group but only 41% (P = .29) lower in the postdebut group compared with the unvaccinated group. Compared with postdebut vaccination, predebut vaccination was associated with an 82% (P = .08) reduction in HPV-16/18 prevalence.
Only 38% of ever-eligible participants were vaccinated, increasing to 56% when restricted to those eligible for RV. However, only 21% (95% CI, 14%-28%) of vaccinated, RV-eligible female adults reported receiving their first dose by age 12 years per ACIP recommendations (mean age at first vaccination dose, 14.5 [95% CI, 14.1-14.8] years). Among these adults, 33% were vaccinated before and 23% after sexual debut. Thus, 41% of vaccinated participants received postdebut vaccination.
Differences by race and ethnicity were negligible (6% of participants were Asian; 20%, Hispanic; 14%, non-Hispanic Black; 55%, non-Hispanic White; and 5%, other groups). Proportions of vaccinated Asian and White participants were slightly higher than those of Black and Hispanic participants (57% and 58% vs 54% and 52%; P = .22). Similar proportions of participants were vaccinated before sexual debut (32%-35%).” -
2) Is The HPV Vaccine Really Safe To Use?
- The HPV vaccine is one of the most studied vaccines ever!
Despite claims from anti-vaccine folks that the vaccine is dangerous, it has an exceptionally strong safety record. No drug or vaccine is completely safe, but all the data indicates that any injuries caused by the HPV vaccine are extremely rare. I have compiled this information below.
As of January 1, 2025, 191 claims for HPV vaccine injuries have been compensated by the U.S. Court of Claims through the federal Vaccine Injury Compensation Program (VICP). To put this in perspective, we can compare this number to the total number of HPV vaccinations administered.
Assuming 38.6% of the U.S. population (estimated at 330 million) received at least one dose of the HPV vaccine, approximately 127,380,000 vaccinations were administered (in fact, most of the people vaccinated have gotten either two or three shots). This means that the ratio of successful claims to vaccinations is at most 1.5 per million, or 0.00015%.
It's important to note that while 965 claims have been filed to the VICP for HPV vaccine-related injuries and deaths, only 191 have been compensated so far. This compensation does not necessarily imply that the vaccine caused the injury in all cases, but rather that the court found the claims met the criteria for compensation under the program's guidelines.
———————————————————————————————————————————————————
Merck, the maker of the HPV vaccine, was sued by a number of plaintiffs alleging that the HPV vaccine made by Merck caused numerous injuries. According to Dorit Reiss, "On March 11, 2025, a federal district court judge granted Merck’s motion for summary judgment in the multi-district litigation against Gardasil, essentially ending the litigation. The judge found that plaintiffs’ warning defects claims could not be brought because Merck did not have new information on which to base warning doctors that HPV vaccines cause postural orthostatic tachycardia syndrome (POTS) or primary ovarian insufficiency (POI). In fact, the judge’s findings strongly suggest that such evidence as existed supported the absence of causation." This covered some 200 cases looking for damages.
This is the best explanation I have seen for why there simply isn't any evidence that Gardasil causes either POTS or POI.
Dorit Rubenstein Reiss: Court grants summary judgment in Gardasil litigation.
———————————————————————————————————————————————————
The Cochrane Library, a well respected database of reviews for all areas of the biomedicine, looked in 2018 at the safety of the HPV vaccines (all the different versions) in retrospective. Their review, Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors, concluded that the HPV vaccine was indeed safe. You can read their summary conclusions here, or download the entire detailed analysis from their website (same link).
The largest single study on the safety of the vaccine was published after the Cochrane library review above, in July, 2020. It looked at over nine million doses of the vaccine given to boys and girls in Australia over an 11 year period. Serious side effects were extremely rare. The most common significant side effect, one that is seen with other vaccines as well, was fainting (syncope) after getting the injection. Even then, the rate was about only 7 to 29 occurrences per 100,000 doses given. Rates for the most serious side effects seen were as follows (shown as the number of cases, followed by the number of events per 100,000 doses):
Anaphylaxis: 30 (0.32)
Guillain-Barre syndrome: 5 (0.05)
Postural orthostatic tachycardia syndrome: 13 (0.14)
Autoimmune disease: 13 (0.14)
Primary ovarian insufficiency: 12 (0.17)
Complex regional pain syndrome: 4 (0.04)
Venous thromboembolism: 3 (0.03)
Expressed as per million doses, the incidence of serious adverse events ranged from 0.3 to 3.2. Note: not all cases are clinically confirmed, and causality is not assumed. Put another way, just because these individuals developed these symptoms does NOT mean that they were caused by the vaccine. It’s only an association. Many of these did not show up until weeks or months following vaccination.
Phillips, A. et al Adverse events following HPV vaccination: 11 years of surveillance in Australia. Vaccine https://doi.org/10.1016/j.vaccine.2020.06.039 FREE download.
—————————————————————————————————————————————————
Here are some earlier studies that also show the HPV vaccine is very safe:
In Sept. 2020 Danish researchers published a paper looking to see if there was any association between 4-valent HPV vaccine and the development of syndromes with autonomic dysfunction, such as chronic fatigue syndrome, complex regional pain syndrome, and postural orthostatic tachycardia syndrome in girls in Denmark. Their study could find no linkage of HPV vaccination with any of these syndromes.
Hiviid, A, et al Association between quadrivalent human papillomavirus vaccination and selected syndromes with autonomic dysfunction in Danish females: population based, self-controlled, case series analysis. BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m2930 (Published 02 September 2020) FREE download
—————————————————————————————————————————————————
In Nov. 2019, three papers were published in the journal Pediatrics that were focused on the safety of the 9-valent HPV vaccine (the most currently available HPV vaccine).
Their conclusion: the HPV vaccine is remarkably safe.
Here’s what the scientists found:
The first study used data from the Vaccine Safety Datalink system:
“During 105 weeks of surveillance, 838, 991 doses of 9vHPV were administered. We identified unexpected statistical signals for 4 adverse events: appendicitis among boys 9 to 17 years old after dose 3; pancreatitis among men 18 to 26 years old; and allergic reactions among girls 9 to 17 years old and women 18 to 26 years old after dose 2. On further evaluation, which included medical record review, temporal scan analysis, and additional epidemiological analyses, we did not confirm signals for any adverse events.
Conclusions: After 2 years of near real-time surveillance of 9vHPV and several pre-specified adverse events, no new safety concerns were identified.”
Donahue JG, et al. Near Real-Time Surveillance to Assess the Safety of the 9-Valent Human Papillomavirus Vaccine. Pediatrics. 2019 Nov 18;. doi: 10.1542/peds.2019-1808. [Epub ahead of print] PubMed PMID: 31740498.
The second study analyzed post-licensure surveillance reports to the Vaccine Adverse Event Reporting System (VAERS):
Conclusions: “No new or unexpected safety concerns or reporting patterns of 9vHPV with clinically important AEs were detected. The safety profile of 9vHPV is consistent with data from prelicensure trials and from postmarketing safety data of its predecessor, the quadrivalent human papillomavirus vaccine.”
Shimabukuro TT, et al. Safety of the 9-Valent Human Papillomavirus Vaccine. Pediatrics. 2019 Nov 18;. doi: 10.1542/peds.2019-1791. [Epub ahead of print] PubMed PMID: 31740500.
The third paper was a commentary about the value of the HPV vaccine:
“Wherever vaccination campaigns against vaccine-preventable cancers have launched, the rates of the pre-cancerous cervical lesions related to the human papillomavirus (HPV) have been reduced.
For many generations, people have wished for a vaccine that would offer protection against cancer.
Curiously, such a vaccine is now readily available but reluctance to administer or to accept the vaccine has kept HPV immunization rates far below those of other routinely recommended vaccines.
The time has come for all vaccine administrators and parents to understand that the availability of the 9-valent human papillomavirus vaccine (9vHPV) is one end of a remarkable journey of discovery and progress to develop a safe and effective vaccine to prevent suffering and death from common cancer.”
Meissner HC. From Peyton Rous to the HPV Vaccine: A Journey of Discovery and Progress. Pediatrics. 2019 Nov 18;. doi: 10.1542/peds.2019-2345. [Epub ahead of print] PubMed PMID: 31740499.
In a nationwide cohort study, with more than 440,000 doses of human papillomavirus (HPV) vaccines administered to young women, no evidence was found to support an association between HPV vaccination and serious adverse events using both cohort analysis and self-controlled risk interval analysis.
Published by the British Medical Journal on January 29, 2021, this nationwide study of girls aged 11-14 years in South Korea, who received HPV, Japanese encephalitis, and tetanus, diphtheria, and acellular pertussis vaccines in 2017, two complementary study designs were used to investigate the association between HPV vaccination and serious adverse events.
Yoon, D. et al Association between human papillomavirus vaccination and serious adverse events in South Korean adolescent girls: nationwide cohort study. BMJ 2021; 372 doi: https://doi.org/10.1136/bmj.m4931 (Published 29 January 2021) Cite this as: BMJ 2021;372:m4931
—————————————————————————————————————————————————
But wait, there’s more! According to the Global Advisory Committee on Vaccine Safety (GACVS), which is a part of the World Health Organization,
“Since licensure in 2006, over 270 million doses of HPV vaccines have been distributed. GACVS first reviewed the safety data in 2007 and subsequently in 2008, 2009, 2013, 2014, and 2015. Early on, the Committee was presented signals related to anaphylaxis and syncope (fainting). The risk of anaphylaxis has been characterized as approximately 1.7 cases per million doses, and syncope was established as a common anxiety or stress-related reaction to the injection. No other adverse reactions have been identified and GACVS considers HPV vaccines to be extremely safe.
Further safety data have been generated recently from Denmark, the United Kingdom and the United States of America and a comprehensive literature review has been conducted, prompting GACVS to review these new findings. Among the new data were studies looking at Guillain-Barré syndrome (GBS). The Committee has already assessed GBS as a signal and noted discrepant findings. Epidemiological studies assessing the risk of GBS following HPV vaccination have been published. including population cohort studies from Denmark and Sweden. In 2017, in response to an online publication from France suggesting an increased risk, a large self-controlled case-series study from the UK was conducted, based on a population where 10.4 million doses were administered. This most recent study found no significant increased risk for GBS after any dose of vaccine, in any of several risk periods assessed or for either vaccine brand. In addition, GBS was specifically selected as an outcome in studies from the US using the Vaccine Adverse Events Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). GACVS was presented with new data from VAERS following 60 million distributed doses, and the VSD data with over 2.7 million doses administered until the end of 2015. No association between HPV vaccine and GBS was identified. Both the UK and US studies concluded, based on their respective data, that a risk of >1 case of GBS per million doses of vaccine could now be excluded.
In addition, GACVS was presented with new studies assessing other safety concerns, again from the US, as well as from Denmark. These studies included examination of specific outcomes that included complex regional pain syndrome (CRPS), postural orthostatic tachycardia syndrome (POTS), premature ovarian insufficiency, primary ovarian failure, and a further look at the risk of venous thromboembolism. With now large population level data from several countries, the Committee saw no new evidence for a causal association between HPV vaccine and those conditions. While safety data from Denmark and Sweden for >3 million women aged 18–44 years showed an apparent increased risk for celiac disease, the investigators considered that, most likely, this represented an unmasking of an existing condition during the vaccination visit rather than a causal association. Overall the study did not raise any other autoimmune safety issues of concern.
As HPV vaccine is often administered during potential childbearing years it is important to establish the safety profile in pregnant women when inadvertent administration occurs. To date no safety concerns have arisen during the pre-licensure clinical trials or in post-licensure surveillance. These reassuring data now include a recent national cohort study from Denmark that assessed 540,805 pregnancies. In addition, new data from the VSD for >92 000 eligible pregnancies were presented to the Committee. No adverse obstetric, birth or structural abnormality outcomes were observed. Inadvertent administration of HPV vaccine during pregnancy has no known adverse outcomes in either mother or infant.
CRPS and POTS continue to be presented as case reports in association with HPV vaccination, particularly from Denmark and Japan. These were initially assessed by GACVS in 2015. These conditions include a spectrum of diverse symptoms, making assessment using administrative health collections challenging. In June 2017, new data from Japan that assessed cases with diverse symptoms, including pain and motor dysfunction, were presented to the Committee. The cases were identified from a nationwide epidemiological survey involving multiple hospital medical departments of various disciplines including pain, neurology, rheumatology, paediatrics and psychiatry/psychosomatic medicine. These complex syndromes manifested in both sexes, although were more common in girls, and occurred in both vaccinated and unvaccinated individuals. The Committee concluded that since their last review, there is still no evidence to suggest a causal association between HPV vaccine and CRPS, POTS or the diverse symptoms that include pain and motor dysfunction.
Also in 2017, the WHO commissioned a systematic review of serious adverse events (SAEs) following HPV vaccines. A draft was presented to GACVS at the meeting. Using the GRADE system to systematically assess the quality of evidence, the quality of evidence in the studies was considered high across randomized controlled trials. The outcomes considered were all SAEs, medically significant conditions, new onset of chronic diseases, and deaths. Data for 73,697 individuals were reviewed. Lower level studies were excluded in favour of the large body of higher level evidence available. For all outcomes, the evidence from randomized controlled trials was supported by good quality cohort studies, with no difference in rates of selected SAEs between exposed and unexposed to HPV vaccine observed.
There are now accumulated safety studies that include several million persons and which compare the risks for a wide range of health outcomes in vaccinated and unvaccinated subjects. However, despite the extensive safety data available for this vaccine, attention has continued to focus on spurious case reports and unsubstantiated allegations. The Committee continues to express concern that the ongoing unsubstantiated allegations have a demonstrable negative impact on vaccine coverage in a growing number of countries, and that this will result in real harm. While ongoing monitoring and collection of robust data are important to maintain confidence, one of the challenges associated with the continued generation of data is that artefacts will be observed, which could pose further challenges for communication when taken in haste, out of context, and in the absence of the overall body of evidence.
GACVS discussed the importance of ensuring that immunization policy-makers and other stakeholders have ready access to articulate summaries of the vaccine safety information, to assist in evidence-based decision-making. One concrete step will be to update the HPV adverse reaction rate sheet, to reflect the most recent evidence available.
Where HPV vaccination programmes have been implemented effectively, the benefits are already very apparent. Several countries that have introduced HPV vaccines to their immunization programme have reported a 50% decrease in the incidence rate of uterine cervix precancerous lesions among younger women. In contrast, the mortality rate from cervical cancer in Japan, where HPV vaccination is not proactively recommended, increased by 3.4% from 1995 to 2005 and is expected to increase by 5.9% from 2005 to 2015. This acceleration in disease burden is particularly evident among women aged 15–44 years. Ten years after introduction, global HPV vaccine uptake remains slow, and the countries that are most at risk for cervical cancer are those least likely to have introduced the vaccine. Since licensure of HPV vaccines, GACVS has found no new adverse events of concern based on many very large, high quality studies. The new data presented at this meeting have strengthened this position.”
If all of this hasn’t convinced you, check out this comprehensive compilation of HPV Vaccine Safety and Effectiveness 2006 - 2019 from Ireland’s National Immunization Office and see if that does the trick. The evidence is overwhelming.
If you’re specifically concerned about stories linking the HPV vaccine to autoimmune diseases, take a look at this article from Dr. Paul Offit in which he reviews alleged autoimmune harms caused by the HPV vaccine. There is no linkage between the two. As one report concluded, “Investigators found no statistically significant differences between the vaccinated and unvaccinated groups in the incidence of immune thrombocytopenia, autoimmune hemolytic anemia, systemic lupus erythematosus (SLE), rheumatoid arthritis, juvenile rheumatoid arthritis, type 1 diabetes, Hashimoto disease, Graves disease, multiple sclerosis, acute disseminated encephalomyelitis, Guillain-Barré Syndrome (GBS), neuromyelitis optica, optic neuritis, or uveitis.”
The Skeptical Raptor weighed in on the safety of the HPV vaccine, and shows it is supported by overwhelming scientific evidence.
Here is a review article that focuses in on the benefits and harms associated with the HPV vaccine from 2020. Note that the specific vaccines have changed since the first one was introduced in 2006 (from bivalent to quadravalent to nonavalent) and that while this time frame may appear to be long, the long latency period following HPV infection means that much of the data we’d like to see will take decades to acquire. Also, the data analyzed here was very limited: it covers only a three year period of study reports obtained from the European Medicines Agency and GlaxoSmithKline from 2014 to 2017. Post study interpretations of the data are also confounding. The bottom line: The HPV vaccines did not significantly increase fatal harms or serious harms.
Jorgensen, L. et al Benefits and harms of the human papillomavirus (HPV) vaccines: systematic review with meta-analyses of trial data from clinical study reports. BMC Systematic Reviews. -
3) Has the Vaccine Reduced HPV Infections, Genital Warts, And Cancers?
The short answer is YES for all of these questions!
A recent study looked at a decline in cervical precancers (which often lead to cervical cancer) in young women in the US. During 2008–2022, cervical precancer incidence decreased 79% and higher-grade precancer incidence decreased 80% among screened women aged 20–24 years, the age group most likely to have been vaccinated. More details can be found in the report below, and also here: CDC report adds to evidence that HPV vaccine is preventing cervical cancer in U.S. women
Gargano, J.W. et al Trends in Cervical Precancers Identified Through Population-Based Surveillance — Human Papillomavirus Vaccine Impact Monitoring Project, Five Sites, United States, 2008–2022. CDC MMRW Feb. 27, 2025
This was for cervical precancers. How about cervical cancer itself in the US? We have data on that as well. Researchers calculated cervical cancer mortality rates of women younger than 25 from 1992-2021. The team divided data into 3-year periods, noting a “gradual decline in cervical cancer deaths of almost 4%” which brought deaths to .02 per 100,000 people from 2013-2015. The death rate for cervical cancer continued to trend downward with “a dramatic reduction in mortality over just 60%,” arriving at .007 deaths per 100,000 according to the 2019-2021 data. Researchers noted a continued positive shift toward lower cervical cancer rates beyond 2021, with a 12% per year decline and 65% reduction overall. The decline is likely due to both vaccination against HPV, which causes cervical cancer, as well as more screening and finding cervical precancers, which if treated properly do not develop into cervical cancer.
Dorali, P. et al Cervical Cancer Mortality Among US Women Younger Than 25 Years, 1992-2021. JAMA. Published online November 27, 2024. doi:10.1001/jama.2024.22169
Next, let's look at two older papers from the UK, showing that the vaccine not only prevents cervical cancer, it also prevents CIN3 cervical pre-cancers as well!
In English girls offered the HPV vaccine at age 12 and/or 13 years, adjusted age-standardized rates of cervical cancer aud CIN3 in the extended follow-up period were a respective 83.9% and 94.3% lower than in those never offered HPV vaccination. As a result of this, the HPV vaccine prevented an estimated 687 cervical cancers and 23,192 cases of CIN3 by 2020. The highest rates of averted cancer and precancerous lesions were still observed in women living in the most socioeconomically deprived areas, but the vaccination program substantially reduced rates in women at all socioeconomic levels. You can read more about this historic study here.
Falcaro, M. et al Effect of the HPV vaccination programme on incidence of cervical cancer and grade 3 cervical intraepithelial neoplasia by socioeconomic deprivation in England: population based observational study. BMJ 2024;385:e077341 http://dx.doi.org/10.1136/ bmj-2023-077341
The most recent study from Scotland also looked at the effectiveness of the HPV vaccine at preventing cervical cancer. Researchers looked at the health records of all women born between 1988 and 1996 who were eligible for cancer screening, about 450,000 women. Of that group, 40,000 were vaccinated between the ages of 12 and 13, and 124,000 received the vaccines at or after 14 years of age. The remaining women, nearly 300,000, were not vaccinated.
No cases of cervical cancer were found among the women who were vaccinated before they turned 14, even if they had only received one or two doses of the vaccine rather than the full, three-dose protocol. Also noteworthy is that women who received the three-dose protocol between the ages of 14 and 22 also benefited significantly. While some cases of cervical cancer were recorded in this group, the incidence (3.2 cases per 100,000 women) was two and a half times lower than among unvaccinated women (8.4 cases per 100,000 women). It should be noted that the actual type of HPV vaccine changed during the years of this study. Until 2012, the vaccine in use was the bivalent Cervarix, targeting HPV 16 and 18. Then the quadrivalent Gardasil (which added in two strains of HPV that cause genital warts) was administered until 2023, when the nonavalent Gardasil 9 was introduced.
Palmer, TJ et al Invasive cervical cancer incidence following bivalent human papillomavirus vaccination: a population-based observational study of age at immunization, dose, and deprivation. Journal Natl. Cancer Inst . 2024 Jan 22:djad263. doi: 10.1093/jnci/djad263
As this paper from the journal Nature points out, elimination of cervical cancer is dependent on vaccination of individuals across all socioeconomic groups.
Malagon, T. et al Epidemiology of HPV-associated cancers past, present and future: towards prevention and elimination. Nat Rev Clin Oncol (2024). https://doi.org/10.1038/s41571-024-00904-z
————————————————————————————————————————————————————————————————————————
The largest analysis to date for the effectiveness of the HPV vaccine was published in The Lancet on June 26, 2019 on behalf of the HPV Vaccine Impact Study Group. It provided substantial evidence of efficacy. As the article states, “This updated systematic review and meta-analysis includes data from 60 million individuals and up to 8 years of post-vaccination follow-up. Our results show compelling evidence of the substantial impact of HPV vaccination programmes on HPV infections and CIN2+ among girls and women, and on anogenital warts diagnoses among girls, women, boys, and men. Additionally, programmes with multi-cohort vaccination and high vaccination coverage had a greater direct impact and herd effects.”
Drolet, M. et al. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta-analysis. DOI:https://doi.org/10.1016/S0140-6736(19)30298-3
Here are some of the most prominent results that came from identifying 1702 potentially eligible articles for this systematic review and meta-analysis, and included 65 articles in 14 high-income countries: 23 for HPV infection, 29 for anogenital warts, and 13 for CIN2+.
After 5-8 years of vaccination, the prevalence of HPV 16 and 18 decreased significantly by 83% among girls aged 13-19 years, and decreased significantly by 66% among women aged 20-24 years.
The prevalence of HPV 31, 33, and 45 decreased significantly by 54% among girls aged 13-19 years.
Anogenital wart diagnoses decreased significantly by 67% among girls aged 15-19 years, decreased significantly by 54% among women aged 20-24 years, and decreased significantly by 31% among women aged 25-29 years.
Among boys aged 15-19 years anogenital wart diagnoses decreased significantly by 48% and among men aged 20-24 years they decreased significantly by 32%.
After 5-9 years of vaccination, CIN2+ decreased significantly by 51% among screened girls aged 15-19 years and decreased significantly by 31% among women aged 20-24 years.
INTERPRETATION:
This updated systematic review and meta-analysis includes data from 60 million individuals and up to 8 years of post-vaccination follow-up. The results show compelling evidence of the substantial impact of HPV vaccination programs on HPV infections and CIN2+ among girls and women, and on anogenital warts diagnoses among girls, women, boys, and men. Additionally, programs with multi-cohort vaccination and high vaccination coverage had a greater direct impact and herd effects.
The effectiveness of the HPV vaccine against genital warts has now been confirmed by a recent meta-analysis:
Lukács, A., et al. The quadrivalent HPV vaccine is protective against genital warts: a meta-analysis. BMC Public Health 20, 691 (2020). https://doi.org/10.1186/s12889-020-08753-y FREE download
—————————————————————————————————————————————————————————
Modeling data suggests that the HPV vaccine may be able to greatly reduce the incidence of cervical cancer.
“These findings emphasise the importance of acting immediately on three fronts to scale up vaccination, screening, and treatment for pre-invasive and invasive cervical cancer. In the next 10 years, a one-third reduction in the rate of premature mortality from cervical cancer in LMICs is possible, contributing to the realisation of the 2030 UN SDGs. Over the next century, successful implementation of the WHO elimination strategy would reduce cervical cancer mortality by almost 99% and save more than 62 million women’s lives.
Canfell,K. et al Mortality impact of achieving WHO cervical cancer elimination targets: a comparative modeling analysis in 78 low-income and lower-middle-income countries. The Lancet. Published online January 30, 2020 https://doi.org/10.1016/S0140-6736(20)30157-4 FREE download
—————————————————————————————————————————————————————————
Interestingly, and not surprisingly, women who have been vaccinated against HPV are more likely than unvaccinated women to take part in cervical cancer screening. “According to the study, women who received at least one dose of the HPV vaccine were 34% more likely to undergo cervical cancer screenings than those who were unvaccinated. The researchers found that the rate of cancer screenings increased as the dose of HPV vaccination increased, and that fully vaccinated individuals were the most likely to undergo screenings. The study also revealed that cancer screening rates were down, overall, during this 10-year period. Overall, findings reveal that 49.8% of women underwent cervical cancer screenings.”
Ba, D., et al. (2021) Cervical cancer screening varies by HPV vaccination status among a National Cohort of privately insured young women in the United States 2006–2016. Medicine. doi.org/10.1097/MD.0000000000027457.
—————————————————————————————————————————————————————————
A landmark Finnish study looked at HPV infection rates in 60,000 girls divided into three groups: unvaccinated; girls-only vaccinated, and both girls and boys vaccinated. The vaccine used was the original Cervarix vaccine, which only targeted two of the most oncogenic strains, 16 and 18. The researchers then followed up with the girls four and eight years after the vaccination to test for 16 different types of genital HPV — HPV 16/18/31/45, the high-oncogenic types, and 12 other types carrying lower cancer risk. In the group with both girls and boys vaccinated, a 50% vaccination coverage per year cohort was sufficient to nearly eliminate the occurrence of the two high-oncogenic HPV types targeted by the vaccine. When the vaccine was just given to girls, the uptake needs to be extremely high (around 90%) to reach the same virus elimination results. By immunizing boys as well the virus has no reservoir to hide in. In addition, HPV45 depletion was observed only in the vaccine group that included boys and girls. No strain depletion was seen in the other two groups. Note that with vaccination protocols in the real world, the percentage of vaccinated who are boys vs girls, and the exact vaccine used (which targeted either two, four, or nine strains of the virus), results may differ from location to location. This may eventually lead to changes to cervical cancer screening protocols since it's believed that nearly all cases of cervical cancer are caused by oncogenic HPV strains. Strain replacement should also occur at the other sites that develop cancer following HPV infection: the back of the throat; the anus, the vagina, the vulva, and the penis.
Because the current vaccine being used targets nine different strains (seven oncogenic, and two that cause genital warts), it's likely that the use of the newer vaccine will speed up the loss of oncogenic strains. One key point: vaccinating both girls and boys greatly accelerates the elimination of the highly oncogenic strains of HPV.
According to this article, “Girls-only vaccination for HPV herd immunity requires 90% of girls to be vaccinated year on year since only half of the population is being protected, but immunizing boys starts to protect the other half of the population and the virus has nowhere to go,” Margaret Stanley, emeritus professor of epithelial biology at the University of Cambridge, who was not involved in the study, wrote in a commentary provided via the Science Media Centre.
At the same time, the samples showed that other HPV types closely related to those targeted by the vaccine had replaced the initial targets. This is not surprising, said Pimenoff: When you have significant variety in a virus type, as with HPV, removing a subset of it leaves a niche that is free to be easily occupied by the remaining strains, which have evolved in a similar way.
Pimenoff, V.N. et al Ecological diversity profiles of non-vaccine-targeted HPVs after gender-based community vaccination efforts. Cell Host & Microbe 31, 1921–1929, November 8, 2023.
———————————————————————————————————————————————————
The news surrounding the HPV vaccine gets better and better.
We already know the vaccine prevents infection with the virus. Because of that, it can actually prevent at least six different types of cancer in men and women. So what’s new? Pregnant women who have been vaccinated against HPV are less likely to suffer from serious pregnancy-related complications. Which complications? Incidences of pre-eclampsia, water breaking early, and antepartum hemorrhage (bleeding after 24 weeks) were significantly reduced in women who had been vaccinated against the virus compared to unvaccinated women.
The data was compiled by the University of Aberdeen on 9,200 women.
Xiaoqian Xu et al, The impact of human papillomavirus (HPV) vaccination on the risk of adverse obstetric outcomes: a data linkage study. European Journal of Obstetrics & Gynecology and Reproductive Biology (2025). DOI: 10.1016/j.ejogrb.2025.114678
———————————————————————————————————————————————————
A new study in April 2026 showed that the HPV vaccine is associated with a significant reduction in oropharyngeal cancer cancers cases arising in boys and young men who were vaccinated between the ages of 9 to 26. This is an actual reduction in the number of cancer cases, not just infections. This is global data and is not just tied to one country.
Kitano, T and Yoshida, S. Nine-Valent Human Papillomavirus Vaccination and Related Cancers in Males. JAMA Oncol
Published Online: April 9, 2026 doi: 10.1001/jamaoncol.2026.0496I’ve broken out the data on a country/regional basis below:
Let’s look first at Australia, the worldwide leader in HPV vaccination
The quadrivalent HPV vaccine led to a 70 per cent reduction in anal strains of HPV in gay and bisexual men. The HYPER2 study found that there was a significant reduction in all four vaccine-preventable genotypes in gay/bisexual men aged 16-20 years following the introduction of the vaccine for boys in 2013. The vaccine covers four genotypes: 6/11/16/18. Genotypes 16/18 cause about 70 per cent of cervical and anal cancers.
This is the first study to show that the implementation of the gender-neutral program can reduce high-risk anal HPV and potentially reduce the incidence of anal cancer in gay and bisexual men.
Chow, E. et al Prevalence of human papillomavirus in young men who have sex with men after the implementation of gender-neutral HPV vaccination: a repeated cross-sectional study. Lancet infectious Diseases DOI: 10.1016/S1473-3099(20)30687-3
—————
The prevalence in Australia of the four HPV types included in the quadrivalent Gardasil vaccine decreased from 22.7% in 2005-07 to 7.3% in 2010-12 to 1.5% in 2015 among women 18-24 years old. That is a 93.4% decrease in HPV types since the introduction of Gardasil in Australia.
Source: Malachek et al Very Low Prevalence of Vaccine Human Papillomavirus Types Among 18- to 35-Year Old Australian Women 9 Years Following Implementation of Vaccination. The Journal of Infectious Diseases, Volume 217, Issue 10, 23 April 2018, Pages 1590–1600. https://doi.org/10.1093/infdis/jiy075
—————
In the first four to five years after vaccination was started in Australia, precancerous abnormalities decreased by 34 per cent in 20–24 year-olds, which means these young women will be at a much lower lifetime risk of ever developing cervical cancer. A reduction in precancerous abnormalities (some of which will go away on their own) means a reduction in the various treatments used to remove these abnormalities, including the loop electrosurgical excision (LEEP) or other cone biopsy procedures, cryosurgery, laser surgery, and even hysterectomy.
Read more at https://www.cancercouncil.com.au/blog/australian-success-story-hpv-vaccine/#HhtSXA7s0SJ8Wwpx.99
In one study of 15-24 year olds, the incidence of genital warts decreased 85% in women and 71% in men following introduction of the HPV vaccine in Australia.
Source: Ali H et al Decline in in-patient treatments of genital warts among young Australians following the national HPV vaccination program. BMC Infect Dis. 2013 Mar 18;13:140. doi: 10.1186/1471-2334-13-140.
—————
In a different study, researchers saw a 58% reduction in genital wart diagnoses in females and a 45% reduction in heterosexual male individuals after the introduction of the HPV vaccination program in 2007. The largest reduction in genital warts was observed in younger individuals, and there was a decreasing magnitude of reduction with increasing age.
Source: Chow, E.P.F. et al Effect on genital warts in Australian female and heterosexual male individuals after introduction of the national human papillomavirus gender-neutral vaccination programme: an analysis of national sentinel surveillance data from 2004–18. The Lancet Infectious Diseases. DOI:https://doi.org/10.1016/S1473-3099(21)00071-2
—————
Want more proof of the effectiveness of the HPV vaccine? There was also a decrease in the incidence of genital warts in young heterosexual men in Australia, even before boys were added to the vaccination program. This illustrates just how effective the vaccination of girls has been in reducing HPV levels in both sexes. Read more about this here.
—————
But wait, there’s even more. HPV also causes a rare disease known as recurrent respiratory papillomatosis (RRP), which can be diagnosed in both children (juvenile onset) and adults (where it may be acquired via sexual transmission, and not present since birth). It is associated with HPV strains 6 and 11 (these are the virus types that cause genital warts, not cancer). Children born with RRP typically develop symptoms of hoarseness and can develop a raspy voice, a chronic cough, and severe breathing problems during their toddler years. It’s treated by surgeries to remove the HPV lesions from the throat, and because it’s virally caused, these lesions can recur. The incidence of this disease is quite rare; only a small fraction of those infected with the virus will develop this condition. In Australia, which has a very high rate of HPV vaccine usage, the incidence of RRP (or more specifically juvenile onset RRP) was impacted by the vaccine. Rates declined from 0.16 per 100000 in 2012 to 0.02 per 100000 in 2016 (P = .034). Novakovic, D. et al. A Prospective Study of the Incidence of Juvenile-Onset Recurrent Respiratory Papillomatosis After Implementation of a National HPV Vaccination Program. J Infect Dis. 2018 Jan 4;217(2):208-212. doi: 10.1093/infdis/jix498.
Here’s a further look at the data from Australia on the treatment of RRP showing the reduction in this disease following HPV vaccine administration.
Brotherton, J. et al. Reduced rates of juvenile onset recurrent respiratory papillomatosis in Australia after implementation of a national HPV vaccination program. Archives of Diseases in Childhood Vol. 103, 2020.
—————
The introduction of the HPV vaccine in Australia in 2007 may have prevented 2000 Australian babies being born premature over eight years. Karen Canfell, director of research at Cancer Council NSW, said the research showed a correlation across the population between vaccine coverage of 60-80 per cent and a fall in premature births, low birth weight and other adverse pregnancy outcomes. "What is estimated is in this group of women, aged 37 or less, there’s around a 3.2 per cent decline in premature delivery," Professor Canfell said. "That might not sound very much but we estimate that is equivalent to around 2000 premature births being prevented."
The vaccine was also correlated with a 9.8 per cent fall in births that are small for gestational age. "We know there is a small risk of adverse pregnancy outcomes resulting from treating pre-cancerous lesions and we know that the vaccines result in the reduction in those lesions, and so everything is backed up in terms of this being an effect that we would expect.”
Yuill, S. et al The Journal of Infectious Diseases, jiaa106, https://doi.org/10.1093/infdis/jiaa106
—————
Finally, a study of men who have sex with men (MSM) found that the quadrivalent HPV vaccine led to reduction in anal, penile, and oral quadrivalent vaccine-targeted genotypes occurred in young MSM following the implementation of a school-based gender-neutral HPV vaccination program.
Chow, E.P. Prevalence of human papillomavirus in young men who have sex with men after the implementation of gender-neutral HPV vaccination: a repeated cross-sectional study.
Lancet Infectious Diseases DOI:https://doi.org/10.1016/S1473-3099(20)30687-3 May 2021Data from the US shows that the HPV vaccine is working:
A recent study looked at a decline in cervical precancers (which often lead to cervical cancer) in young women in the US. During 2008–2022, cervical precancer incidence decreased 79% and higher-grade precancer incidence decreased 80% among screened women aged 20–24 years, the age group most likely to have been vaccinated. More details can be found in the report below, and also here: CDC report adds to evidence that HPV vaccine is preventing cervical cancer in U.S. women
Gargano, J.W. et al Trends in Cervical Precancers Identified Through Population-Based Surveillance — Human Papillomavirus Vaccine Impact Monitoring Project, Five Sites, United States, 2008–2022. CDC MMRW Feb. 27, 2025
This was for cervical precancers. How about cervical cancer itself in the US? We have data on that as well. Researchers calculated cervical cancer mortality rates of women younger than 25 from 1992-2021. The team divided data into 3-year periods, noting a “gradual decline in cervical cancer deaths of almost 4%” which brought deaths to .02 per 100,000 people from 2013-2015. The death rate for cervical cancer continued to trend downward with “a dramatic reduction in mortality over just 60%,” arriving at .007 deaths per 100,000 according to the 2019-2021 data. Researchers noted a continued positive shift toward lower cervical cancer rates beyond 2021, with a 12% per year decline and 65% reduction overall. The decline is likely due to both vaccination against HPV, which causes cervical cancer, as well as more screening and finding cervical precancers, which if treated properly do not develop into cervical cancer.
Dorali, P. et al Cervical Cancer Mortality Among US Women Younger Than 25 Years, 1992-2021.
An older study looked at the rate at which women in the US under the age of 25 die from cervical cancer. Cervical cancer is cause by HPV infections, so as more girls get immunized against the virus, we would expect the rates of infection, cervical cancer, and cervical cancer deaths to decline. In this study, the rate of deaths in this cohort declined by 62%. While the exact cause of this decline isn't known, it's highly likely that it is due to the vaccines that these girls received when they were about 10 years old.
Dorali, P. et al Cervical Cancer Mortality Among US Women Younger Than 25 Years, 1992-2021. JAMA. Published online November 27, 2024. doi:10.1001/jama.2024.22169
In 2024 an abstract was presented at the American Society of Clinical Oncology meeting with real world data on the effectiveness of the original HPV vaccine. What did that data show?
"Results from a new research study show that the human papillomavirus (HPV) vaccine lowers the chances of developing cancer caused by HPV, including head and neck cancer in men and boys and cervical cancer in women and girls.
The most common cancer caused by HPV is cervical cancer. Since the approval of the HPV vaccine in the United States in 2006, many studies have shown that the HPV vaccine reduces the risk of cervical cancer. However, other cancers can be caused by HPV, including head and neck cancer, anal cancer, penile cancer, vulvar cancer, and vaginal cancer. This study compared the risk of developing all HPV-related cancers in people who received the HPV vaccine with those who did not.
This study is a retrospective analysis. This type of research compares 2 or more groups of people by looking at data that has already been collected in the past. This study looked at data from 3,413,07 people ages 9 to 39 years old who had a medical visit where any vaccine was given between January 1, 2010, and December 31, 2023. The study population was divided into 2 groups: people who had received the HPV vaccine at least 5 years earlier (1,706,539 people) and those who had not received the HPV vaccine (1,706,538 people). Their average age was 21 years, 56% were women, and 53% were White, 21% were Black, 5% were Asian, 0.4% were American Indian or Alaskan Native, 0.4% were Native Hawaiian, and 21% were of other or unknown race.
Men and boys vaccinated for HPV had a lower risk of developing all HPV-related cancers compared to unvaccinated men and boys. In this group, there were 3.4 cases of HPV-related cancer for every 100,000 vaccinated patients compared to 7.5 cases of HPV-related cancer for every 100,000 unvaccinated patients. HPV vaccination also lowered the risk of developing head and neck cancers among men and boys. There were 2.8 cases of head and neck cancer for every 100,000 vaccinated patients, compared to 6.3 cases for every 100,000 unvaccinated patients.
Women and girls vaccinated for HPV also had a lower risk of developing all HPV-related cancers. In this group, there were 11.5 cases of HPV-related cancer for every 100,000 vaccinated patients, compared to 15.8 cases for every 100,000 unvaccinated patients. Women and girls who had received HPV vaccination also had a lower risk of developing cervical cancer. There were 7.4 cases of cervical cancer for every 100,000 vaccinated patients, compared to 10.4 cases for every 100,000 unvaccinated patients. Vaccinated women who had never had abnormal findings during a Pap test were also less likely to develop precancerous dysplasia of the cervix and undergo invasive procedures. Vaccinated women did not have a significantly lower risk of developing head and neck cancer or vaginal cancer when compared to those who did not receive the vaccine.
Because many HPV-related cancers are more common in older adults, research will continue to study outcomes in people older than 39 years of age.
What does this mean for patients? The HPV vaccine lowers the risk of developing HPV-related cancers in men and women, especially head and neck cancer in men and cervical cancer in women."
Here's another way of looking at the data from medical reporter Matthew Herper: "the data being presented at ASCO are based on the rates of HPV in a giant database of electronic health records from 90 million patients collected by TriNetX, a private company in the business of using such data to conduct observational studies. The researchers were able to compare roughly 1.7 million patients vaccinated for HPV with roughly the same number of age-matched control patients with no prior HPV vaccination. A total of 56% were female, 53% were white, 21% were Black/African American, with a mix of people of other backgrounds represented.
There are problems with this setup that actually make it tougher for the vaccine. For instance, some patients who had cervical lesions were known to get the vaccine after the lesions had shown up, and people might be getting the vaccine after they had already been infected with HPV, which takes many, many years to cause cancer. It’s also possible that some people who were included in the control group somehow got the vaccine and it wasn’t recorded, which would make the vaccine appear less effective.
Still, the results were dramatic. Vaccinated males had 3.4 cases of HPV-linked cancer per 100,000 patients compared to 7.5 per 100,000 unvaccinated patients. Vaccinated females had 11.5 cases per 100,000 patients compared to 15.8 per 100,000 unvaccinated patients."
——————————————————————————————————————————————————————————
The latest data in 2021 from the US is stunningly strong, showing just how effective the HPV vaccine has been at preventing infection by the virus. Data that was collected through 2018 showed that infections with four strains of HPV targeted by the first available HPV vaccines showed an 88% reduction in the number of infected females aged 14 to 19 and an 81% reduction in women age 20 to 24 compared with before vaccination efforts started in 2006. The data also show evidence of indirect protection of unvaccinated females through herd immunity effects in these age groups.
Rosenblum, H.G. Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine — United States, 2003–2018. MMWR Weekly / March 26, 2021 / 70(12);415–420.
Similar data has been published here (May 2022): Rosenblum HG, et al. Human papillomavirus vaccine impact and effectiveness through 12 years after vaccine introduction in the United States, 2003 to 2018. Ann Intern Med 2022; DOI: 10.7326/M21-3798.
Earlier data:
As a result of the introduction of the HPV vaccine in 2006, we are starting to see declines in the prevalence of the HPV types that the vaccine targets. In one study, the prevalence of vaccine-type HPV decreased >90% in vaccinated women, demonstrating high effectiveness in a community setting, and >30% in unvaccinated women, providing evidence of herd protection.
Kahn et al Substantial Decline in Vaccine-Type Human Papillomavirus (HPV) Among Vaccinated Young Women During the First 8 Years After HPV Vaccine Introduction in a Community. Clinical Infectious Disease 63, 1281 (2016) DOI: 10.1093/cid/ciw533
Even better, here’s a paper with actual data showing the effect of herd immunity with the HPV vaccine in young women in the US that was done 2006-2017. Among the women who were vaccinated, 4-valent vaccine–type HPV detection decreased from 35% to 6.7%. Among women who were NOT vaccinated, 4-valent vaccine–type HPV detection decreased from 32.4% to 19.4%. (The 4-valent vaccine refers to the original Gardasil vaccine, which covered four HPV strains. It was replaced with Gardasil 9, which covers nine HPV strains.)
Spinner, C. et al Human Papillomavirus Vaccine Effectiveness and Herd Protection in Young Women. Pediatrics. 2019;143(2):e20181902
In a separate study from Kaiser Permanente Northwest, researchers looked at which strains of HPV in were found in cytology specimens from women aged 20-29 years screened for cervical cancer at Kaiser Permanente Northwest in 2007, and in two vaccine era periods: 2012-2013 and 2015-2016. Detection and typing used L1 consensus PCR with hybridization for 37 types, including quadrivalent vaccine types (HPV 6/11/16/18). Within 9-10 years of vaccine introduction, the prevalence of HPV strains that the quadrivalent vaccine protects against decreased 78% among 20-24 year-olds and 38% in 25-29 year-olds. There were declines in BOTH vaccinated and unvaccinated women, showing evidence of direct and herd protection.
Markowitz, L.E. Declines in HPV vaccine type prevalence in women screened for cervical cancer in the United States: Evidence of direct and herd effects of vaccination. Vaccine. 2019 May 31. pii: S0264-410X(19)30626-7. doi: 10.1016/j.vaccine.2019.04.099
In another study (findings presented at the CDC’s Epidemic Intelligence Service, or EIS, conference in April 2019), researchers used the National Health and Nutrition Examination Survey to evaluate the quadrivalent Gardasil vaccine (4vHPV)-type prevalence among 4,674 females in the prevaccine (2003–2006) and vaccine (2013–2016) eras overall and by race and ethnicity. Their results showed that among females aged 14 to 19 years, 53.9% received more than one dose of vaccine, including 52.6%, 58.1% and 59.5% of non-Hispanic white, non-Hispanic black and Mexican American females, respectively. Among women aged 20 to 24 years, coverage with more than one dose was 51.5%, including 58.5%, 45% and 33.8% in non-Hispanic white, non-Hispanic black (45%) and Mexican Americans, respectively.
In the younger cohort, the 4vHPV-type prevalence decreased from 11.5% to 1.8% from the pre-vaccine to vaccine era, with steep declines seen in all three groups. In the older cohort, prevalence decreased from 18.5% to 5.3%.
Also as a result of the introduction of the HPV vaccine in 2006, we are starting to see declines in the incidence of cervical pre-cancers both in those that are vaccinated as well as those who aren’t via herd immunity in both white and black women:
“In 10,206 cases, the proportion and estimated number of cases of HPV16/18-positive CIN2+ declined from 52.7% (1,235 cases) in 2008 to 44.1% (819 cases) in 2014 (P < 0.001). Declining trends in the proportion of HPV16/18-positive CIN2+ were observed among vaccinated (55.2%–33.3%, P < 0.001) and unvaccinated (51.0%–47.3%, P = 0.03) women; ages 18–20 (48.7%–18.8%, P = 0.02), 21–24 (53.8%–44.0%, P < 0.001), 25–29 (56.9%–42.4%, P < 0.001), and 30–34 (49.8%–45.8%, P = 0.04) years; CIN2 (40.8%–29.9%, P < 0.001) and CIN2/3 (61.8%– 46.2%, P < 0.001); non-Hispanic white (59.5%–47.9%, P < 0.001) and non-Hispanic black (40.7%– 26.5%, P < 0.001).”
McClung et al Trends in Human Papillomavirus Vaccine Types 16 and 18 in Cervical Precancers, 2008– 2014 . Cancer Epidemiology, Biomarkers & Prevention DOI: 10.1158/1055-9965.EPI-18-0885
In addition, the CDC has recorded a decrease in high-grade cervical lesions (CIN2+) during the 2008-2016 period. The rate of CIN2+ per 100,000 women declined significantly in women aged 18–19 years and 20–24 years (many of whom had been given the HPV vaccine) and increased significantly in women aged 40–64 years (none of whom would have been vaccinated). Much of this decrease in cervical pre-cancers is being attributed to the HPV vaccine.
McClung et al Estimated Number of Cases of High-Grade Cervical Lesions Diagnosed Among Women — United States, 2008 and 2016. Morbidity and Mortality Weekly Report (MMWR) Weekly / April 19, 2019 / 68(15);337–343.
In another study, Anil Chaturvedi at the National Cancer Institute and his colleagues looked at a nationwide survey on HPV infections in the years following the vaccines’ introduction. Nearly 14,000 adults took part in the survey, conducted from between 2009 and 2016. Over those years, HPV vaccination rates increased from zero to 5.8 per cent in men and from 7.3 per cent to 15.1 per cent in women. During this period, the prevalence of the types of HPV that the vaccine prevents infection with dropped from 2.7 per cent to 1.6 per cent in men who had not been vaccinated. This represented a 37 per cent drop among the unvaccinated adult men. The authors suggested that herd immunity was protecting these men, which “likely arises from increased levels of female HPV vaccination in the US population.”
Chaturvedi, A.K. et al Prevalence of Oral HPV Infection in Unvaccinated Men and Women in the United States, 2009-2016. JAMA. 2019; 322(10):977-979. doi: 10.1001/jama.2019.10508
Finally, and most importantly, as a result of the introduction of the HPV vaccine in 2006, we are starting to see declines in the prevalence of cervical cancer in the young women first given the vaccine. The 4-year average annual incidence rates for cervical cancer in 2011–2014 were 29% lower than that in 2003–2006 (6.0 vs 8.4 per 1,000,000 people) among females aged 15–24 years, and 13.0% lower among females aged 25–34 years.
Guo et al Cervical Cancer Incidence in Young U.S. Females After Human Papillomavirus Vaccine Introduction. American Journal of Preventive Medicine Volume 55, Issue 2, 197–204, 2018. https://doi.org/10.1016/j.amepre.2018.03.013
A study analyzing all cervical cancer cases diagnosed in people 15-24 years and tracked in the US, District of Columbia and Puerto Rico found there was a 29% drop after the vaccine was introduced in 2006. This decrease was statistically significant. It’s unusual to have cervical cancer diagnosed in such young women, but as more time passes, we will have more and more data that shows a reduction in actual cervical cancer cases.
Guo, F. et al Cervical Cancer Incidence in Young U.S. Females After Human Papillomavirus Vaccine Introduction. American Journal of Preventive Medicine 55, no. 2 (2018): 197–204. https://doi.org/10.1016/j.amepre.2018.03.013.
In addition, we have another study using the 4-valent version of the HPV-vaccine (original Gardasil). The study compared the incidence of HPV infection for strains covered by the vaccine for both vaccinated and unvaccinated girls. Among vaccinated women, HPV detection decreased from 35% to 6.7% (80.9% decline; odds ratio 0.13, 95% confidence interval 0.08 to 0.22). Among women who were unvaccinated, HPV detection decreased from 32.4% to 19.4% (40% decline; odds ratio 0.50, 95% confidence interval 0.26 to 0.97). This latter effect is attributed to herd immunity; even non-vaccinated girls show evidence of reduced infection rates.
Spinner, C. et al Human Papillomavirus Vaccine Effectiveness and Herd Protection in Young Women. Pediatrics February 2019, 143 (2) e20181902; DOI: https://doi.org/10.1542/peds.2018-1902. FREE download.
Another study examined incidence rates of cervical squamous cell carcinoma (SCC) and adenocarcinoma (AC) among women aged 15–29 years diagnosed during 1999–2017 using population-based cancer registry data covering 97.8% of the U.S. population. The report concluded since the introduction of the HPV vaccine, both SCC and AC cervical cancer incidence rates declined among women aged 15–20 years, a group not typically screened for cervical cancer, which may suggest HPV vaccine impact.
Mix, J.M. et al Assessing Impact of HPV Vaccination on Cervical Cancer Incidence among Women Aged 15–29 Years in the United States, 1999–2017: An Ecologic Study. Cancer Epidemiology, Biomarkers, and Prevention DOI: 10.1158/1055-9965.EPI-20-0846 Published January 2021.
In yet another study, data released in 2021 showed that the boys getting at least one dose of the quadrivalent HPV vaccine before age 18 years has a vaccine effectiveness of 85% against penile infection with 4vHPV-type HPV in men who have sex with men (MSM) and in transgender women.
Winer R.L. et al Pre-adult HPV vaccination yields dramatic decline in penile infection risk. J Infect Dis, 28 July 2021 doi: 10.1093/infdis/jiab390.
In a 2022 study, the effectiveness of the HPV vaccine in the US has was demonstrated by comparing women who were born in the 1980s vs those born in the 1990s. Those born in the earlier decade has a higher prevalence of cancer causing strains of HPV compared to women born in the later decade (who were vaccinated against HPV starting in 2016).
The HPV vaccine was recommended for routine use starting in 2006 for young women aged 9 to 26 years old.“
To assess the effectiveness of the vaccine, a study published in JAMA Health Forum compared the probability of women born in the 1980s and 1990s being diagnosed with HPV. The researchers found that women born in the 1990s were at a lower risk of HPV. Data from 2 cycles of the National Health and Nutritional Examination Survey (2005-2006 and 2015-2016) were used for this study. Infection prevalence of HPV types 16 and 18 were estimated. Data analyses were performed.
Results: There were 2698 women aged 18 to 26 years (mean [SD] age of 21.5 [2.7] years) and 32% White. Prevalence of HPV-16/18 was significantly lower in women born in the 1990s (5.6%; 95% CI, 4.0%-7.2%) compared with the women born in the 1980s (12.5%; 95% CI, 10.2%-14.7%).”
This study also provided clear evidence of herd immunity, protecting women who had not yet been vaccinated.
Shahmoradi, Z et al Prevalence of Human Papillomavirus Infection Among Women Born in the 1990s vs the 1980s and Association With HPV Vaccination in the US. JAMA Health Forum. 2022;3(8):e222706. doi:10.1001/jamahealthforum.2022.2706
HPV-IMPACT
The CDC maintains a program focused on monitoring the effectiveness of the HPV vaccine. It’s called the Human Papillomavirus Vaccine Impact Monitoring Project (HPV-IMPACT). According to the CDC website:
“Measuring the impact (such as reduction in HPV-related precancers) of the HPV vaccine on health outcomes is a critical but challenging public health priority. Of highest importance is the impact of the vaccine on reducing the burden of cervical cancer, which is the most common HPV-related cancer in women. However, since it takes many years for HPV infection to progress to invasive cancer, measuring vaccine impact on cervical cancer is difficult and can take decades. Instead, we can monitor high-grade cervical lesions that are likely to progress to invasive cancer if left untreated as early indicators of vaccine impact. In this surveillance project, we monitor these cervical lesions among women age 18 and older in five different communities around the United States.
The CDC collects demographic and clinical information from laboratory and medical records for every woman who has a high-grade cervical lesion identified. For women aged 18-39 years who have a high-grade cervical lesion identified, we collect additional information, such as insurance, cervical cancer screening history, and vaccination history. Additionally, archived tissue specimens are obtained and sent to CDC for HPV type testing for 37 HPV types, including those targeted by HPV vaccines.
The main objectives of HPV-IMPACT are to:
Monitor trends in overall incidence of high-grade cervical lesions over time in women aged 18-39 years;
Monitor prevalence and distribution of HPV types in women aged 18-39 years with high-grade cervical lesions;
Describe the demographic, clinical, and HPV type characteristics among patients with high-grade cervical lesions;
Estimate and monitor trends in cervical cancer screening among residents of the catchment areas; and
Estimate the proportion of patients with high-grade cervical lesions who received the HPV vaccine, and estimate vaccine effectiveness.
The HPV-IMPACT project is a collaboration between two groups at CDC: the Viral Vaccine Preventable Diseases Branch in the Division of Viral Diseases, and the Chronic Viral Diseases Branch in the Division of High-Consequence Pathogens and Pathology.”
—————————————————————————————————————————————————————————
In another meta-analysis, researchers evaluated the efficacy of HPV vaccination in preventing recurrent cervical intraepithelial neoplasia (CIN) 2 or greater after surgical excision.
The data suggest that the HPV vaccine may be able to greatly reduce cervical dysplasia recurrence risk. Researchers compared recurrence rates of 1,360 women who received HPV vaccination after surgical excision for recurrent cervical dysplasia with those of 1,624 women who received placebo or surgery alone. “Recurrence of CIN 2 or greater occurred within 6-48 months in 115 women (3.9%) overall; however, recurrence was significantly lower for vaccinated women: 26 of 1,360 women (1.9%) vs 89 of 1,624 unvaccinated women (5.9%) (relative risk [RR] 0.36 95% CI 0.23-0.55). The risk of CIN 1 or greater was also significantly lower with adjuvant HPV vaccination, occurring in 86 of 1,360 vaccinated women (6.3%) vs 157 of 1,624 unvaccinated women (9.7%) (RR 0.67 95% CI 0.52-0.85). Thirty-five women developed recurrent CIN 2 or greater lesions specific to HPV 16,18; nine received adjuvant vaccination (0.9%) vs 26 who were unvaccinated (2.0%) (RR 0.41 95% CI 0.20-0.85).”
Lichter, K.et al Adjuvant Human Papillomavirus Vaccine to Reduce Recurrent Cervical Dysplasia in Unvaccinated Women: A Systematic Review and Meta-analysis. Obstet Gynecol. 2020 Jun;135(6):1489. doi: 10.1097/AOG.0000000000003937.Data from the Nordic countries shows that the HPV vaccine is working:
A study was done in Sweden to see if the HPV vaccine could prevent not just cervical pre-cancers, but cervical cancer itself. They looked at a demographic of over 1.6 million girls and women who had gotten the HPV vaccine. “The cumulative incidence of cervical cancer was 47 cases per 100,000 persons among women who had been vaccinated and 94 cases per 100,000 persons among those who had not been vaccinated. After adjustment for age at follow-up, the incidence rate ratio for the comparison of the vaccinated population with the unvaccinated population was 0.51 (95% confidence interval [CI], 0.32 to 0.82). After additional adjustment for other covariates, the incidence rate ratio was 0.37 (95% CI, 0.21 to 0.57). After adjustment for all covariates, the incidence rate ratio was 0.12 (95% CI, 0.00 to 0.34) among women who had been vaccinated before the age of 17 years and 0.47 (95% CI, 0.27 to 0.75) among women who had been vaccinated at the age of 17 to 30 years. Conclusion: Among Swedish girls and women 10 to 30 years old, quadrivalent HPV vaccination was associated with a substantially reduced risk of invasive cervical cancer at the population level.”
Lei, J. et al HPV Vaccination and the Risk of Invasive Cervical Cancer. N Engl J Med 2020; 383:1340-1348. DOI: 10.1056/NEJMoa1917338
As a result of the introduction of the HPV vaccine, we now have data from women immunized for 2, 4, 6, 8, and 10 years. The data show that there were exactly zero cases at any time point of HPV 16/18-related cervical intraepithelial neoplasia 2 (CIN2) or worse (CIN3, adenocarcinoma in situ, or actual cervical cancer) among women receiving the quadrivalent HPV vaccine at the start of the study. There were also zero cases of vulvar or vaginal cancer in this same study.
Kajer et al A 12-Year Follow-up on the Long-Term Effectiveness of the Quadrivalent Human Papillomavirus Vaccine in 4 Nordic Countries. Clinical Infectious Diseases (2018) 66, 339-345.
Similarly, another study showed that the rate of cervical cancer in HPV vaccine immunized girls dropped to zero compared to non-vaccinated girls.
Luostarinen, T. Vaccination Protects Against Invasive HPV-Associated Cancers. Int. J. Cancer 142, 2186-2187 (2018) FREE download.
Another study looked at HPV prevalence in 23 year old young women who had been given the quadrivalent HPV vaccine at age 14. Prevalence of any high-risk (HR) HPV was 35%; only 0.9% were positive for vaccine HPV-types 16/18 while the remaining 34% were positive for other HR HPV. When comparing with pre-vaccination prevalence data, HPV-16/18 decreased by 95%; RR=0.05 (95% CI 0.04-0.06), while other HR HPV remained fairly constant; RR=0.88 (95% CI 0.82-0.94) and RR=0.95 (95% CI 0.88-1.03), respectively. One third of women vaccinated as girls with the quadrivalent HPV-vaccine were HR HPV-positive at time of first invitation to screening. Vaccine HPV-types 16 and 18 were almost eliminated, while the prevalence of non-vaccine HR HPV-types remained constant.
Lynge, E. et al. Prevalence of High-Risk Human Papillomavirus After HPV-vaccination in Denmark. Int. J Cancer . 2020 Jun 16. doi: 10.1002/ijc.33157.
—————————————————————————————————————————————————————————
A landmark Finnish study looked at HPV infection rates in 60,000 girls divided into three groups: unvaccinated; girls-only vaccinated, and both girls and boys vaccinated. The vaccine used was the original Cervarix vaccine, which only targeted two of the most oncogenic strains, 16 and 18. The researchers then followed up with the girls four and eight years after the vaccination to test for 16 different types of genital HPV — HPV 16/18/31/45, the high-oncogenic types, and 12 other types carrying lower cancer risk. In the group with both girls and boys vaccinated, a 50% vaccination coverage per year cohort was sufficient to nearly eliminate the occurrence of the two high-oncogenic HPV types targeted by the vaccine. When the vaccine was just given to girls, the uptake needs to be extremely high (around 90%) to reach the same virus elimination results. By immunizing boys as well the virus has no reservoir to hide in. In addition, HPV45 depletion was observed only in the vaccine group that included boys and girls. No strain depletion was seen in the other two groups. Note that with vaccination protocols in the real world, the percentage of vaccinated who are boys vs girls, and the exact vaccine used (which targeted either two, four, or nine strains of the virus), results may differ from location to location. This may eventually lead to changes to cervical cancer screening protocols since it's believed that nearly all cases of cervical cancer are caused by oncogenic HPV strains. Strain replacement should also occur at the other sites that develop cancer following HPV infection: the back of the throat; the anus, the vagina, the vulva, and the penis.
Because the current vaccine being used targets nine different strains (seven oncogenic, and two that cause genital warts), it's likely that the use of the newer vaccine will speed up the loss of oncogenic strains. One key point: vaccinating both girls and boys greatly accelerates the elimination of the highly oncogenic strains of HPV.
According to this article, “Girls-only vaccination for HPV herd immunity requires 90% of girls to be vaccinated year on year since only half of the population is being protected, but immunizing boys starts to protect the other half of the population and the virus has nowhere to go,” Margaret Stanley, emeritus professor of epithelial biology at the University of Cambridge, who was not involved in the study, wrote in a commentary provided via the Science Media Centre.
At the same time, the samples showed that other HPV types closely related to those targeted by the vaccine had replaced the initial targets. This is not surprising, said Pimenoff: When you have significant variety in a virus type, as with HPV, removing a subset of it leaves a niche that is free to be easily occupied by the remaining strains, which have evolved in a similar way.
Pimenoff, V.N. et al Ecological diversity profiles of non-vaccine-targeted HPVs after gender-based community vaccination efforts. Cell Host & Microbe 31, 1921–1929, November 8, 2023.Data from Scotland shows that the HPV vaccine is working:
The most recent study in Scotland looked at the effectiveness of the HPV vaccine at preventing cervical cancer. Researchers looked at the health records of all women born between 1988 and 1996 who were eligible for cancer screening, about 450,000 women. Of that group, 40,000 were vaccinated between the ages of 12 and 13, and 124,000 received the vaccines at or after 14 years of age. The remaining women, nearly 300,000, were not vaccinated.
No cases of cervical cancer were found among the women who were vaccinated before they turned 14, even if they had only received one or two doses of the vaccine rather than the full, three-dose protocol. Also noteworthy is that women who received the three-dose protocol between the ages of 14 and 22 also benefited significantly. While some cases of cervical cancer were recorded in this group, the incidence (3.2 cases per 100,000 women) was two and a half times lower than among unvaccinated women (8.4 cases per 100,000 women). It should be noted that the actual type of HPV vaccine changed during the years of this study. Until 2012, the vaccine in use was the bivalent Cervarix, targeting HPV 16 and 18. Then the quadrivalent Gardasil (which added in two strains of HPV that cause genital warts) was administered until 2023, when the nonavalent Gardasil 9 was introduced.
Palmer, TJ et al Invasive cervical cancer incidence following bivalent human papillomavirus vaccination: a population-based observational study of age at immunization, dose, and deprivation. Journal Natl. Cancer Inst . 2024 Jan 22:djad263. doi: 10.1093/jnci/djad263
———————————————————————————————————————————————————————————————————————————
In an earlier study, the introduction of the bivalent HPV vaccine (Cervarix) shows that routine vaccination of girls aged 12-13 led to a dramatic reduction in preinvasive cervical disease. The study showed that compared with unvaccinated women born in 1988, vaccinated women born in 1995 and 1996 showed an 89% reduction in prevalent cervical intraepithelial neoplasia (CIN) grade 3 or worse (from 0.59% to 0.06%; an 88% reduction in CIN grade 2 or worse (from 1.44% to 0.17%), and a 79% reduction in CIN grade 1 (from 0.69% to 0.15%). Younger age at immunization was associated with increasing vaccine effectiveness: 86% for CIN grade 3 or worse for women vaccinated at age 12-13 compared with 51% for women vaccinated at age 17. Evidence of herd protection against high grade cervical disease was found in unvaccinated girls in the 1995 and 1996 cohorts.
Palmer, TJ et al Prevalence of cervical disease at age 20 after immunisation with bivalent HPV vaccine at age 12-13 in Scotland: retrospective population study. British Medical Journal (2019); 365:1161 doi: 10.1136/bmj.l1161 (FREE paper)
It appears that the bivalent HPV vaccine can not only prevent infection against the targeted strains of HPV (16; 18); it can also prevent infection with closely related non-targeted strains (31; 33; 45).
More great news about these safe and effective vaccines!Data from England shows that the HPV vaccine is working:
A 2021 study out of England showed just how incredibly effective the HPV vaccine is at preventing both cervical cancer and precancers when given to young girls. The earlier the vaccine is administered, the fewer cases of cervical cancer and precancers were found:
“The estimated relative reduction in cervical cancer rates by age at vaccine offer were 34% (95% CI 25–41) for age 16–18 years (school year 12–13), 62% (52–71) for age 14–16 years (school year 10–11), and 87% (72–94) for age 12–13 years (school year 8), compared with the reference unvaccinated cohort. The corresponding risk reductions for CIN3 were 39% (95% CI 36–41) for those offered at age 16–18 years, 75% (72–77) for age 14–16 years, and 97% (96–98) for age 12–13 years.“
The authors estimated that by June 30, 2019 there had been 448 (339–556) fewer than expected cervical cancers and 17,235 (15,919–18,552) fewer than expected cases of CIN3 in vaccinated cohorts in England.
Interpretation:
The authors observed a substantial reduction in cervical cancer and incidence of CIN3 in young women after the introduction of the HPV immunisation programme in England, especially in individuals who were offered the vaccine at age 12–13 years. The HPV immunisation programme has successfully almost eliminated cervical cancer in women born since Sept 1, 1995.
Falcaro, M. et al. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. DOI:https://doi.org/10.1016/S0140-6736(21)02178-4
Published Nov. 3, 2021 in The Lancet.
—————————————————————————————————————————————————————————
A report released by Public Health England reviewed surveillance data from outcomes of a national HPV vaccination program, which began in 2008. The report looked at incidence of HPV infection of the reproductive tract in sexually active 16-24 year-old females. As is the case with many viruses, HPV has many subtypes, some of which are more likely to be associated with aggressive cancers (subtypes 16 and 18 as well as 31, 33, and 45) and others are more likely to be associated with RRP infections and genital warts (subtypes 6 and 11). Until 2012, the bivalent (HPV 16/18) vaccine (CervarixR) was administered as a three-dose regimen. In years since then, the quadrivalent (HPV 16/18/6/11) (GardasilR) has been the standard vaccine administered in the U.K. as well as the U.S. as a two-dose regimen. Cervical cancer is due to HPV 16 or HPV 18 in up to 80% of cancers.
The report analyzed results of over 18,000 vulvovaginal culture specimens obtained from sexually active 16-24-year-old females undergoing chlamydia screening, collected between 2010 and 2018. There was significant decline in HPV infection rates in all subtypes in all age groups. Those who had been vaccinated more recently showed more reduction in HPV 6/11 than those who did not receive coverage for these strains in the earlier years of vaccination. Most notable was that the prevalence of HPV 16/18 in the 16-18-year-old cohort declined from 8.2% in 2010 to 0.0% in 2018. In the older groups, there was less decline (from 14% to 0.7% in 19-21-year-olds and 16.4% to 2.6% in 22-24-year-olds), but all reductions were statistically significant.
Surveillance of type-specific HPV in sexually active young females in England, to end 2018. HPR Volume 14 Number 2 Advanced Access report published 22 January 2020. FREE download.Data from Canada shows that the HPV vaccine is working:
A study from British Columbia looked at the incidence of cervical pre-cancers in girls who had, or had not, gotten the HPV vaccine. “The overall reduction post-vaccination for CIN2 and 3 in women 16‐23 years was respectively 62% (95% CI 54‐68%) and 65% (95% CI 58‐71%). Age‐specific rates for CIN2 significantly declined for those 18‐22 years of age and for those 19, 20 and 23 years of age for CIN3.”
Donken, R. Declining rates of cervical intraepithelial neoplasia in British Columbia, Canada: An ecological analysis on the effects of the school‐based human papillomavirus vaccination program. https://doi.org/10.1002/ijc.33513-
4) Does The HPV Vaccine Protect Against All Strains Of The Virus?
- Human papilloma viruses share some common structural proteins, but each strain also differs from one another. The vaccine is made against certain proteins that are different on each type of virus and are found on the outside of the virus (the viral shell) because the outside of the virus is what our immune system sees. Because of this, the vaccine only provides protection against a limited number of strains. A vaccine that targeted a protein that is identical in all human papilloma viruses would, in theory, provide protection against all strains, but such a vaccine has yet to be created.
If you want to get into the details about differences between various strains of HPV, take a look at this paper:
Burk et al Human papillomavirus genome variants Virology. 2013 Oct; 445(0): 232–243. doi: 10.1016/j.virol.2013.07.018
——————————————————————————————————————————————————————————
Efforts to create a universal HPV vaccine that would be active against all cancer causing strains are underway. For example, PathoVax LLC has started clinical trials of just such a vaccine that covers at least 18 strains of the virus. These trials are only Stage 1, so it’s going to be awhile before we find out if this vaccine is safe and more effective than Gardasil 9. -
5) Does Infection With One Strain Of HPV Protect You From Other Strains?
- No. You can be infected with multiple strains of HPV at the same time. Being infected with one strain does not provide protection against infection with a different strain. A study was done looking at women who were referred for HPV testing when they were having cells from their cervixes examined. Twenty four percent of the women were positive for HPV infection, and 19 percent of those infected with one strain also harbored a second strain. The overall percentage of women who were infected with at least two strains of HPV was 4.6 percent. "Women who harbor multiple infections are at higher risk for cervical lesions than those ever infected with one type only and should be followed more closely," said Eduardo L. Franco, Dr.PH., professor of epidemiology and oncology, and director, division of cancer epidemiology at McGill University.
The research raises the possibility that in women with multiple infections, their immune systems may be less robust in clearing the infections. HPV 16, the most well known cancer causing strain, was found in 9 percent and 14 percent of single and multiple HPV infections, respectively.In theory the vaccine should prevent someone who is already infected with HPV from being infected by a second strain, providing that the second strain is one of the nine strains that the Gardail 9 vaccine works against. Those who received the earlier vaccines (Cervarix or Gardasil) that only protected against two strains of HPV (16 and 18) or four strains of HPV (16, 18, 6, and 11), respectively, could also get some benefit from the most recent vaccine, Gardasil 9, that provides protection against a total of nine strains.
Having said that, it’s the two most prevalent cancer-causing strains (16 and 18) that are found in the vast majority of HPV-caused cancers. For example, WHO reports that 70 percent of cervical cancers are linked to these two strains. One study estimated that the Gardasil 9 vaccine may prevent an additional 4.2 percent to 18.3 percent of cancers compared to the vaccines targeted at just strains 16 and 18. Thus, there are diminishing returns in getting the newest vaccine if you have already been immunized with the earlier ones. As always, discuss this with your doctor to weigh the pluses and minuses. You may also want to check if your insurance company would pay for new HPV vaccinations if you’ve previously been vaccinated with one of the earlier vaccines. -
6) Can The Vaccine Prevent Oral HPV infections?
- Lorem ipsum dolor sit amet, sapien platea morbi dolor lacus nunc, nunc ullamcorper. Felis aliquet egestas vitae, nibh ante quis quis dolor sed mauris. Erat lectus sem ut lobortis, adipiscing ligula eleifend, sodales fringilla mattis dui nullam. Ac massa aliquet.Yes. A study of more than 2,600 young adults showed that the prevalence of four different types of oral HPV, including two high risk strains (16 and 18), was 88 percent lower in those who had gotten at least one dose of the HPV vaccine compared to those who were not vaccinated.
Take a look at HPV Vaccination Linked to Decreased Oral HPV Infections National Cancer Institute 2017 -
7) Was The HPV Vaccine Tested Against A Saline Control In Clinical Trials?
- Some were, and some were not. There were many trials done to establish the safety and efficacy of the HPV vaccine. Many of the trials were done with additional ingredients (typically, an aluminum adjuvant) in the control group. That is actually the best way to test out vaccines to see if there is a difference between the control and vaccinated groups caused by the immunogen (which in this case is a protein from HPV that evokes the important immune response). Of the many trials done, two of them were done with saline controls. Both showed that the vaccine was both safe and effective. So if anyone tells you that the HPV vaccine trials were done without saline control groups, you can tell them they are wrong, and share these two papers with them.
Reisinger, K.S. et al Safety and persistent immunogenicity of a quadrivalent human papillomavirus types 6, 11, 16, 18 L1 virus-like particle vaccine in preadolescents and adolescents: a randomized controlled trial. Pediatr Infect Dis J. 2007 Mar;26(3):201-9.
Ferris, D. et al Long-term Study of a Quadrivalent Human Papillomavirus Vaccine. Pediatrics Volume 134, Number 3, September 2014 -
8) How Long Is The HPV Vaccine Protective For?
- The exact time period is not known for sure. The most currently used vaccine, Gardasil 9, was only introduced in 2014, so the earliest participants in clinical trials have just been treated for 6-7 years. A report in the journal Lancet showed that vaccine efficacy has been maintained for six years (Lancet. 2017 Nov 11;390(10108):2143-2159. doi: 10.1016/S0140-6736(17)31821-4). A literature review/meta-analysis The Efficacy and Duration of Vaccine Protection Against Human Papillomavirus (Dtsch Arztebl Int. 2014 Sep; 111(35-36): 584–591) showed no loss of long term protection from HPV vaccines.
Mathematical models based on current data estimate that the original Cervarix HPV vaccine will provide full immunity for at least 30 years. According to this article in Science, about the use of virus like particles (VLP) in HPV vaccines, “Trials have shown that nearly everyone vaccinated with that noninfectious VLP develops high levels of HPV-neutralizing antibodies. Those levels decline moderately after 2 years but then remain stable for at least a decade.” The HPV vaccine leads to consistent blood levels of neutralizing antibodies for years on end. According to some scientists, “VLPs trigger production of a different set of B cells called long-lived plasma cells (LLPCs), which reside in the bone marrow and continually produce antibodies specific to different foreign antigens.”
Jon Cohen. Waning immunity: Vaccine protection can fade in months or last a lifetime. Understanding why could lead to more durable immune responses. Science 364 (6437), 224-227. DOI: 10.1126/science.364.6437.224
You can read this article for FREE.
—————
A study from Finland compared Cervarix with Gardasil to see how long of an antibody response was maintained, and against which strains. The results were quite interesting. Researchers analyzed 577 serum samples from the quadrivalent vaccine recipients (Gardasil) and 568 from the bivalent vaccine (Cervarix) recipients. In 681 first-pregnancy serum samples, neutralizing antibodies to HPV6, 16, and 18 were generally found up to 12 years after vaccination. However, 51 (15%) of 339 quadrivalent vaccine recipients had no detectable HPV18 neutralising antibodies 2–12 years after vaccination, whereas all 342 corresponding bivalent vaccine recipients had HPV18 neutralising antibodies
In seropositive quadrivalent vaccine recipients, HPV16 geometric mean titres (GMT) halved by years 5–7 (GMT 3679, 95% CI 2377 to 4708) compared with years 2–4 (6642, 2371 to 13 717). Between 5 and 12 years after vaccination, GMT of neutralising antibodies to HPV16 and 18 were 5·7 times and 12·4 times higher, respectively, in seropositive bivalent vaccine recipients than in the quadrivalent vaccine recipients. Cross-neutralising antibodies to HPV31, 33, 45, 52, and 58 were more prevalent in the bivalent vaccine recipients but, when measurable, sustainable up to 12 years after vaccination with similar GMTs in both vaccine cohorts.
Seroprevalence for HPV16, 31, 33, 52, and 58 significantly correlated with vaccine efficacy against persistent HPV infections in the bivalent vaccine recipients only (rs=0·90, 95% CI 0·09 to 0·99, p=0·037, compared with rs=0·62, 95% CI –0·58 to 0·97, p=0·27 for the quadrivalent vaccine recipients). Correlation of protection with prevalence of neutralizing or cross-neutralizing HPV antibodies was not significant in the quadrivalent vaccine recipients.
Mariz, F.C. et al Sustainability of neutralising antibodies induced by bivalent or quadrivalent HPV vaccines and correlation with efficacy: a combined follow-up analysis of data from two randomised, double-blind, multicentre, phase 3 trials. The Lancet Infectious Diseases DOI:https://doi.org/10.1016/S1473-3099(20)30873 (2021) -
9) Are There Side Effects To Getting The HPV Vaccine?
- As with nearly all vaccines, there are mild side effects associated with getting the HPV vaccine. These usually last a few hours to a day.
According to the World Health Organization, In the arm where the vaccine is given:
“• Pain is felt by about 8 in 10 people.
• Redness or swelling is experienced by about 1 in 4 people.
• Headache: About 1 in 3 people will develop a headache.
Fever:
• Mild fever (100° F/38° C) is experienced by about 1 in 10
people.
• Moderate fever (102° F/39° C) is experienced by about 1 in
65 people.
About one in a million people who receive a vaccine of any kind will experience a strong allergic reaction (such as anaphylactic shock). For this reason, health care providers should ask about allergies before giving a vaccine and advise whether a known allergy is relevant to the specific vaccine being given. The person being vaccinated should stay in the clinic for 15 minutes afterwards for observation.”
There have been claims that HPV causes a number of problems, but these claims have been carefully examined and shown not to be associated with the vaccine.
Source: Adverse Effects of Vaccines: Evidence and Causality (2012) Chapter: 9 Human Papillomavirus Vaccine. Nap.edu. https://www.nap.edu/read/13164/chapter/11#520. Causality judgments from the US Institute of Medicine.Getting the HPV often hurts. This is because this particular vaccine is one of a type of vaccines that is referred to as reactogenic. According to Wikipedia “Reactogenicity events are adverse events that are common and known to occur”, such as a sore arm at the injection site, or a fever. Typically, reactogenicity with vaccines is often observed when the vaccine contains an adjuvant (a chemical additive intended to enhance the recipient's immune response to the vaccine antigen), but it can also occur with non-adjuvanted vaccines. All versions of the HPV vaccine have had added adjuvants, including the one currently available in the U.S., Gardasil 9. -
10) Can I Get Financial Help To Pay For The Vaccine?
- Help is available from several sources:
Medicaid - The Vaccines for Children (VFC) program provides vaccines for children ages 18 years and younger, or who are uninsured, Medicaid-eligible, American Indian or Alaska Native. It also covers those who have health insurance, but are underinsured (i.e. the insurance doesn’t cover any vaccines or doesn’t cover certain recommended vaccines). Underinsured children are eligible to receive vaccines only at federally qualified health centers (FQHCs) or rural health clinics (RHCs). FQHCs and RHCs provide health care to medically underserved areas and meet certain criteria under Medicare and Medicaid programs. If you need help locating an FQHC or RHC, contact your state or city’s VFC program coordinator. There are more than 40,000 healthcare providers in the US enrolled in this program. Click this link to find the VFC provider nearest where you live, or call the CDC at 1-800-CDC-INFO (1-800-232-4636) for assistance.
Children’s Health Insurance Program (CHIP) – State CHIP programs that are separate from their Medicaid programs must cover the CDC’s Advisory Community for Immunization Practices (ACIP)-recommended vaccines for beneficiaries since they are not eligible for coverage under the federal VFC. The HPV vaccine is one covered by ACIP.
The Immunization Grant Program (Section 317 of the Public Health Service Act) provides grants to states and local agencies to increase the availability of vaccines to uninsured adults in the United States. Check with your local health agency to see if the vaccine is available.
If you’re over 18, there’s a program to provide the vaccine to young adults. Merck, the manufacturer of the vaccine, has established the Merck Vaccine Patient Assistance Program (MVPAP), which is funded by Merck for adults 19 to 26 years of age who cannot afford vaccines. It’s a private and confidential program provides vaccines free of charge to eligible adults, primarily the uninsured who, without assistance, could not afford needed vaccines. To qualify you must be 19 to 26 years of age, don’t have health insurance, and can’t afford to pay for the vaccine. Details can be found at Merck Helps by clicking this link. -
11) Is It Safe To Give The Vaccine To Pregnant Women?
- Apparently so, although this has never been tested due to ethical considerations. According to the Global Advisory Committee on Vaccine Safety (GACVS), which is a part of the World Health Organization, “inadvertent administration of HPV vaccine during pregnancy has no known adverse outcomes in either mother or infant.”
-
12) How Many People Need To Be Vaccinated To Prevent A Single Cancer Case?
- The answer to this isn’t known. A 2007 paper by Brisson et al estimated that using the vaccine available at the time (Gardasil, which only protects against four strains of HPV: 16, 18, 6, and 11; only the first two cause cancer), you would have to vaccinate about 324 girls to prevent one case of cervical cancer. This estimate may be good, or it may be bad. It’s based on mathematical modeling. Whatever the number is, it would actually be much better today for two reasons. One, the most recent vaccine, Gardasil 9, protects against five additional cancer causing strains of the virus (31, 33, 45, 52, and 58) compared to Gardasil original. That makes the current vaccine more effective at preventing cancer, although not hugely so since most cases (about 70%) of cervical cancer are thought to be caused by strains 16 and 18. The other thing to keep in mind is that the HPV vaccine not only prevents most cases of cervical cancer in women, it should also prevent most cases of vaginal, vulval, oropharyngeal, and anal cancer as well.
A separate study estimates that the number needed to treat (NNT) for preventing a single case of cervical pre-cancer is 60. Put another way, you need to vaccinate 60 girls to prevent a single case of HPV-caused cervical pre-cancer.
Source: Arbyn M, et al. Prophylactic vaccination against human papilloma viruses to prevent cervical cancer and its precursors. Cochrane Database of Systematic Reviews 2018, Issue 5. Art. No.: CD009069. DOI: 10.1002/14651858.CD009069.
According to the National Cancer Institute, the HPV virus is believed to be responsible for about 70% of cervical cancers, 65 percent of vaginal cancers, 50 percent of vulvar cancers, 95 percent of anal cancers, and 70 percent of oropharyngeal (back of the throat, tonsil, and base of the tongue) cancers.
Data from the CDC indicates that in 2015, oropharyngeal cancers made up only 14% of all HPV-cancers in women. The most prevalent HPV-cancer in women is cervical cancer (48%), followed by anal cancers (18%), vulval cancers (16%), and vaginal cancers (3%).
So overall, the number of girls needed to treat with the most recent vaccine in order to prevent a single case of cancer might be more in the range of about half of the previous estimate, or around 162 girls. But nobody knows for sure.
I have been unable to find any estimates for the number of boys needed to be vaccinated to prevent a single case of oropharyngeal, anal, or penile cancer in men. Since men have an approximately equal number of HPV cancers each year compared to women, the number is likely to be similar.
Reference:
Brisson M et al Estimating the number needed to vaccinate to prevent diseases and death related to human papillomavirus infection CMAJ. 2007 Aug 28; 177(5): 464–468. doi: 10.1503/cmaj.061709
———————————————————————————————————————————————————————————————————————————————
How many individuals need to be vaccinated to prevent a single case of any HPV cancer? A study in 2024 attempted to answer this question by comparing different groups age 27-45 and compared that with the previous standard vaccination group of 9-26 year olds in the United States. The estimated number of individuals that model projected that needed to be vaccinated to prevent a single case of HPV-cancer was 7,670 for those considered "mid-adults;" 3,190 for those who were highly sexually active; and 5,150 for those who recently separated, respectively. Compare this to the ages 9-26 year old group, where only 223 patients need to be vaccinated to prevent a single case of HP-caused cancer.
Laprise JF, Chesson HW, Markowitz LE, Drolet M, Brisson M. Cost-Effectiveness of Extending Human Papillomavirus Vaccination to Population Subgroups Older Than 26 Years Who Are at Higher Risk for Human Papillomavirus Infection in the United States. Ann Intern Med. 2024. doi:10.7326/M24-0421 -
13) Can The Vaccine Cause Autism?
- No. There is absolutely no evidence that the HPV vaccine (or for that matter, any vaccine) causes autism. None at all.
Most of the misinformation about vaccines causing autism have been focused on the MMR vaccine. It doesn’t. Read this article that reviews in great detail why there is no association. It includes references for 140 papers that all support this, including the most recent huge analysis (Measles, Mumps, Rubella Vaccination and Autism: A Nationwide Cohort Study) of more than 650,000 children in Denmark. This Danish study found zero evidence of any association between the MMR vaccine and autism. -
14) When Was The Vaccine First Introduced?
- In the US, the Food and Drug Administration (FDA) has approved three vaccines that prevent infection with disease-causing HPV types: Gardasil®, Gardasil® 9, and Cervarix®. Gardasil was originally introduced in 2006 (for girls only), Cervarix was first marketed in the US in 2009 (again, only for girls), and Gardasil 9 replaced Gardasil in the US in 2014. Up until 2010, the vaccines were only given to girls, after which they started to be given to both boys and girls when it was clearly understood that HPV also causes oral, anal, and penile cancers in men. Cervarix was withdrawn from the US marketplace in 2016 due to low market demand, leaving Gardasil® 9 as the only HPV vaccine for sale in the US.
The two Gardasil vaccines are manufactured by Merck, whereas Cervarix is a product of GlaxoSmithKline. Click this link for information on which countries have licensed Gardasil 9, and this link for which countries had licensed Cervarix. -
15) Is The Vaccine Made From Live Virus?
- No, there is NO live virus in the HPV vaccine, and therefore it is NOT possible to “catch” HPV from the vaccination. HPV vaccines are made by using yeast to generate one of the HPV proteins, called L1, from HPV. The L1 protein is then purified and self-assembles into pentamers (an organized arrangement of five of the protein molecules), and next 72 of the pentamers self-assemble into a structure known as a virus like particle (VLP). Think of the VLP as being like the shell of an egg, but without any yolk or whites contained inside. The VLP are hollow particles that are good at generating an immune response. Scientists at Merck (who manufacture the vaccine) combine VLPs made from L1 proteins from nine different strains of HPV to produce the Gardasil 9 vaccine.
See Conway and Meyers, Replication and Assembly of Human Papillomaviruses. J Dent Res. 2009 Apr; 88(4): 307–317. doi: [10.1177/0022034509333446] -
16) Isn't The Vaccine More Dangerous Than The Risk Of Getting Cancer?
- In a word, no.
Let’s do the math together to answer this question.
For individuals not vaccinated against HPV, the cumulative risk of developing an HPV-associated cancer in any organ was 1.4% in white women, and about 0.98% in white men. Thus, about 1 in 71 white women will develop one of these cancers, and about 1 in 100 white men will. If we focus just on cervical cancer, the estimated lifetime risk for developing cervical cancer is only 0.68%, or about 1 in 147 women.
Howlader, et al SEER cancer statistics review, 1975-2009 (vintage 2009 populations). National Cancer Institute, https://seer.cancer.gov/archive/csr/1975_2009_pops09/.
According to the CDC, “Gardasil 9 is currently the only HPV vaccine available in the United States. From its licensure in December 2014 through December 2017 (four year period), about 29 million doses of Gardasil 9 have been distributed in the U.S. During the same period, VAERS received 7,244 U.S. reports of adverse events following Gardasil 9 vaccination. Overall, 97% were non-serious reports; 3% of reports have been classified as serious.”
The CDC also cautions people about the data contained in the VAERS database, “The Vaccine Adverse Event Reporting System (VAERS) is a national vaccine safety monitoring system co-managed by CDC and FDA. The system accepts adverse event reports following vaccination from vaccine manufacturers, healthcare professionals, and the public. It serves as an early warning system to detect possible safety problems that require further evaluation; however, the safety data the system provides has limitations. VAERS data limitations include reporting biases, inconsistent data quality and completeness, and a lack of unvaccinated comparison groups. Because of these limitations, VAERS generally cannot determine if a vaccine caused a reported adverse event. While some reported adverse events may be caused by vaccination, others may be coincidental and not related to vaccination. Learn more about VAERS and the safety data it provides.”
Many, if not most, of the serious adverse reports are likely NOT related to getting the vaccine, but let’s just go with the numbers as reported. Three percent of the 7,244 adverse events comes out to 217 potentially serious adverse events. With 29 million doses, that comes means that during a three year period there was one serious adverse event for every 133,640 vaccinations. Each person getting the vaccine should have gotten either two or three doses. Let’s average that out at 2.5 doses per person, which means that there will be one person potentially harmed per every 53,456 people vaccinated. Note that the actual number is likely to be higher than this, because a significant number of people never complete the required number of doses.
————————————————————————————————————————————————————————————————
We can expand this dataset in the National Vaccine Injury Compensation Program (VICP) to look at ALL versions of the HPV vaccine over a ten year period:
Number of doses given (2006-2016): 101,405,935
Total compensable claims filed: 288
Number of claims dismissed: 160
Total compensable claims awarded: 128 (this includes concessions, court decisions, and settlements)
This works out to be 0.00126 percent of those vaccinated against HPV filed a claim and were compensated at some level. There were an average of 12 claims paid out each year to those who said they were harmed by the HPV vaccine (again, this court does not require absolute proof to award settlements). Each person getting the vaccine will have gotten either two or three doses. Let’s average that out at 2.5 doses per person, which means that the vaccine fully treated about 40,562,374 individuals. Divide that by 128 awards, and we get one claim awarded for every 316,893 people vaccinated. Note that the actual number is likely to be higher than this, because a significant number of people never complete the required number of doses.
So here’s your choice: about 1 in 71 white women, and 1 in 100 white men will develop an HPV-caused cancer during their lifetimes. Let’s just average this to 1 in 85 white adults will develop one of these cancers.
Bottom line:
You have about a 1 in 85 chance of getting an HPV-caused cancer in your lifetime.
You have about a 1 in 53,456 to 316,893 chance of being seriously harmed by the vaccine.
Put another way, for every person who might possibly have been seriously harmed by the vaccine, there will be 629 to 3,728 men and women who will develop an HPV-preventable cancer sometime during their life.
Keep in mind that there were a total of 43,371 HPV-associated cancers in 2015 in the US: 24,432 cases in women, and 18,939 cases in men. HPV causes oropharyngeal, anal, penile, cervical, vaginal, and vulvar cancers. It also causes painful genital warts. This is why it’s a good idea to vaccinate both girls AND boys against HPV!
The right choice seems pretty obvious to me.
And for those of you wanting to put these numbers in context: there are about 51 people in the US killed (not just struck) by lightning each year, and sharks attack about 19 people over that time frame. This illustrates just how safe the HPV vaccine is; there are only about 12 compensable claims per year.
The HPV vaccine is safer than sharks or lightning.
————————————————————————————————————————————————————————————————
You may have heard that it’s possible to have a life threatening anaphylactic reaction to a vaccine. This is true. However, it’s incredibly rare. The actually rate was 1.31 per million vaccine doses. Yes, it is a one in a million event. The incidence did not vary significantly by age, and there was a nonsignificant female predominance. The onset of symptoms among cases was within 30 minutes (8 cases), 30 to less than 120 minutes (8 cases), 2 to less than 4 hours (10 cases), 4 to 8 hours (2 cases), the next day (1 case), and not documented (4 cases). Epinephrine (like Epi-pen injectors) is an effective antidote for those who have this rare reaction, and all doctors who administer vaccines are trained in spotting this reaction, and for dealing with it.
McNeil, M.M. et al Risk of anaphylaxis after vaccination in children and adults. J Allergy Clin Immunol. 2016 Mar; 137(3): 868–878.
Published online 2015 Oct 6. doi: 10.1016/j.jaci.2015.07.048 FREE download -
17) Is Strain Replacement A Problem With This Vaccine?
- The subject is complicated, and much of the work done to date revolves around mathematical modeling. But how does this operate in the real world, and specifically, with HPV? There has been evidence of strain replacement with other vaccines, but it is highly likely that this mechanism will vary a lot between different types of vaccines. Factors involved include how many replacement strains are available in the population, how many strains the vaccine is effective against, what percentage of the population is vaccinated, the virulence of the various strains, and how communicable is the particular pathogen (in this case, a virus).
In 2023 we finally got at least a partial answer to this question, and it appears to be yes.
A landmark Finnish study looked at HPV infection rates in 60,000 girls divided into three groups: unvaccinated; girls-only vaccinated, and both girls and boys vaccinated. The vaccine used was the original Cervarix vaccine, which only targeted two of the most oncogenic strains, 16 and 18. The researchers then followed up with the girls four and eight years after the vaccination to test for 16 different types of genital HPV — HPV 16/18/31/45, the high-oncogenic types, and 12 other types carrying lower cancer risk. In the group with both girls and boys vaccinated, a 50% vaccination coverage per year cohort was sufficient to nearly eliminate the occurrence of the two high-oncogenic HPV types targeted by the vaccine. When the vaccine was just given to girls, the uptake needs to be extremely high (around 90%) to reach the same virus elimination results. By immunizing boys as well the virus has no reservoir to hide in. In addition, HPV45 depletion was observed only in the vaccine group that included boys and girls. No strain depletion was seen in the other two groups. Note that with vaccination protocols in the real world, the percentage of vaccinated who are boys vs girls, and the exact vaccine used (which targeted either two, four, or nine strains of the virus), results may differ from location to location. This may eventually lead to changes to cervical cancer screening protocols since it's believed that nearly all cases of cervical cancer are caused by oncogenic HPV strains. Strain replacement should also occur at the other sites that develop cancer following HPV infection: the back of the throat; the anus, the vagina, the vulva, and the penis.
Because the current vaccine being used targets nine different strains (seven oncogenic, and two that cause genital warts), it's likely that the use of the newer vaccine will speed up the loss of oncogenic strains. One key point: vaccinating both girls and boys greatly accelerates the elimination of the highly oncogenic strains of HPV.
According to this article, “Girls-only vaccination for HPV herd immunity requires 90% of girls to be vaccinated year on year since only half of the population is being protected, but immunizing boys starts to protect the other half of the population and the virus has nowhere to go,” Margaret Stanley, emeritus professor of epithelial biology at the University of Cambridge, who was not involved in the study, wrote in a commentary provided via the Science Media Centre.
At the same time, the samples showed that other HPV types closely related to those targeted by the vaccine had replaced the initial targets. This is not surprising, said Pimenoff: When you have significant variety in a virus type, as with HPV, removing a subset of it leaves a niche that is free to be easily occupied by the remaining strains, which have evolved in a similar way.
Pimenoff, V.N. et al Ecological diversity profiles of non-vaccine-targeted HPVs after gender-based community vaccination efforts. Cell Host & Microbe 31, 1921–1929, November 8, 2023.
—————————————————————————————————————————————————————————————
Here are some previous efforts to examine this question of strain replacement.
Take a look at Evidence for cross-protection but not type-replacement over the 11 years after human papillomavirus vaccine introduction. Covert et al. Hum Vaccin Immunother. 2019.
Look at theoretical modeling of this phenomenon in Martcheva et al Vaccine-induced pathogen strain replacement: what are the mechanisms?J R Soc Interface. 2008 Jan 6; 5(18): 3–13. doi: 10.1098/rsif.2007.0236
For a look at HPV, see the study by Markowitz et al Prevalence of HPV After Introduction of the Vaccination Program in the United States Pediatrics. 2016 Mar;137(3):e20151968. doi: 10.1542/peds.2015-1968.
Finally, this issue has also been addressed in Murall et al Could the human papillomavirus vaccines drive virulence evolution? Proc Biol Sci. 2015 Jan 7; 282(1798): 20141069. doi: 10.1098/rspb.2014.1069
—————————————————————————————————————————————————————————————
Now to actual data. A new study suggests that HPV vaccination might make women more susceptible than their non-vaccinated peers to HPV genotypes NOT covered by the vaccine.
Although these other HPV gentypes not included in the vaccine are rarer and less aggressive, they can still cause cancer.
The data come from the Costa Rica HPV Vaccine Trial, which involved more than 10,000 women aged 18–25 years. The HPV vaccine used in the trial was Cervarix, from GlaxoSmith Kline. It covers the two leading causes of cervical cancer, HPV 16 and 18, and provides partial protection against three other genotypes. This is an older vaccine; the current vaccine Gardasil 9 used in most developed countries protects against nine different strains of HPV, including seven ones that cause cancer.
“During the period 2004–2005, investigators randomly assigned 3727 women aged 18–-25 years to receive Cervarix and 3739 to a control group that received the hepatitis A vaccine; after 4 years, the control group also received Cervarix and exited the study. They were replaced by an unvaccinated control group of 2836 women. The new control group and the original HPV vaccine group were followed for an additional 7 years.
In years 7–11 of the trial, the investigators found 9.2 additional cervical intraepithelial neoplasias of grade 2 or worse (CIN2+) from HPV types not covered by Cervarix per 1000 vaccinated women in comparison with unvaccinated participants. This corresponds to -71.2% negative vaccine efficacy against CIN2+ lesions of HPV types not covered by the vaccine.
There were 8.3 additional CIN3+ lesions from non-targeted HPV strains per 1000 vaccinated women in comparison with unvaccinated participants, which corresponds to -135% negative vaccine efficacy.
Overall, however, there was a net benefit of vaccination, with 27 fewer CIN2+ lesions when all HPV genotypes ― vaccine covered or not ― were considered per 1000 vaccinated women over the entire 11 years of follow-up.” There were also 8.7 fewer CIN3+ lesions across all genotypes per 1000 vaccinated women, but the benefit was not statistically significant.
Among the study limits, the team was unable to evaluate the effect of clinical unmasking on cervical cancer, because women were treated for high-grade cervical lesions before cases could progress to cervical cancer.”
Vaccinated women "still had long-term absolute reductions in high-grade lesions,”and the net protection "remained considerable, emphasizing the importance of HPV vaccination for cervical cancer prevention.”
Shing, J.Z. et al. Precancerous cervical lesions caused by non-vaccine-preventable HPV types after vaccination with the bivalent AS04-adjuvanted HPV vaccine: an analysis of the long-term follow-up study from the randomised Costa Rica HPV Vaccine Trial. Published:June 13, 2022 The Lancet Oncology DOI:https://doi.org/10.1016/S1470-2045(22)00291-1
The results are likely the first evidence to date of "clinical unmasking" with HPV vaccination, meaning that protection against the strains covered by the vaccine leaves women more prone to attack from other carcinogenic HPV variants. -
18) Can Women Who Have Gotten The Vaccine Skip Cervical Cancer Screening?
- No. The CDC recommends that she should still be screened. Both older versions of the HPV vaccine as well as the current one don’t protect individuals against all HPV types that cause cervical cancer.
Vaccination would certainly reduce the odds of her developing cervical cancer, because the vaccine is directed against the most prevalent cancer causing strains, but it cannot guarantee it.
Not all vaccines, including the HPV vaccine, are 100% effective, so this is another reason to still get screened for cervical cancer. Having said that, the HPV vaccine is among the most effective vaccines, with almost 100% effectiveness against the nine strains covered.
Finally, women who got the vaccine after they became sexually active may not get the full benefit of the vaccine if they had already been exposed to HPV. That’s why screening would still be a good idea for most women.
A study published in 2021 looked at the rates of cervical cancer screening in young women aged 21-29 who either had, or had not, been vaccinated against HPV. The study showed that the unvaccinated women were also less likely to be screened for cervical cancer than the vaccinated women. Among women aged 21 to 29 years who were not vaccinated for HPV, a higher proportion reported never receiving cervical cancer screening compared with vaccinated women (32.2% vs 17.9%; P < .001). Put another way, the women most at risk of getting cervical cancer because they haven’t been vaccinated against HPV were also the ones least likely to be screened.
Sonawane, K. et al Evaluation of Cervical Cancer Screening Uptake and Adherence Among Women Without Human Papillomavirus Vaccination in the US. JAMA Netw Open. 2021;4(10):e2131129. doi:10.1001/jamanetworkopen.2021.31129. FREE Download.
———————————————————————————————————————————————————————————————
Despite the fact that cervical cancer rates have been dropping since the introduction of the HPV vaccine (see all the data in FAQ 3 above), a recent report indicated that there has actually been an increase in late stage (stage IV) cervical cancer in the US during the period of 2001 to 2018. In short, there has been an annual increase in distant stage cervical cancer at a rate of 1.3% per year over this time. How could this happen if overall cervical cancer rates are dropping? It’s not known why this is, but it has been suggested that has occurred due to a decline in cervical cancer screening rates.
“The largest increase is seen in cervical adenocarcinoma with an average annual percent change of 2.9%. After doing an analysis of race, region and age, it was determined that white women in the South aged 40–44 have the highest rise in distant cervical cancer at a rate of 4.5% annually. Using the Behavioral Risk Factor Surveillance System and TeenVax data, compared with Black women, we found that white women have a nearly two-fold higher rate of missed or lack of guideline screening, 26.6% vs 13.8%. White teenagers (13–17 years) have the lowest human papillomavirus vaccination rate at 66.1% compared with others at 75.3%.”
Conclusions: Black women have a higher incidence of late stage disease compared with white women. However, white women have a greater annual increase, particularly in adenocarcinomas. Compared with black women, white women also have lower rates of guideline screening and vaccination.
Francoeur AA, et al The increasing incidence of stage IV cervical cancer in the USA: what factors are related? International Journal of Gynecologic Cancer Published Online First: 18 August 2022. doi: 10.1136/ijgc-2022-003728
———————————————————————————————————————————————————————————————
The effectiveness of the HPV vaccine in the US has also been shown by comparing women who were born in the 1980s vs those born in the 1990s. Those born in the earlier decade has a higher prevalence of cancer causing strains of HPV compared to women born in the later decade (who were vaccinated against HPV starting in 2016).
Shahmoradi, Z et al Prevalence of Human Papillomavirus Infection Among Women Born in the 1990s vs the 1980s and Association With HPV Vaccination in the US. JAMA Health Forum. 2022;3(8):e222706. doi:10.1001/jamahealthforum.2022.2706
The HPV vaccine was recommended for routine use starting in 2006 for young women aged 9 to 26 years old. “
To assess the effectiveness of the vaccine, a study published in JAMA Health Forum compared the probability of women born in the 1980s and 1990s being diagnosed with HPV. The researchers found that women born in the 1990s were at a lower risk of HPV. Data from 2 cycles of the National Health and Nutritional Examination Survey (2005-2006 and 2015-2016) were used for this study. Infection prevalence of HPV types 16 and 18 were estimated. Data analyses were performed.
Results: There were 2698 women aged 18 to 26 years (mean [SD] age of 21.5 [2.7] years) and 32% White. Prevalence of HPV-16/18 was significantly lower in women born in the 1990s (5.6%; 95% CI, 4.0%-7.2%) compared with the women born in the 1980s (12.5%; 95% CI, 10.2%-14.7%).” -
19) Does The US Have A National Goal For HPV Immunization?
- Yes there is, but let’s start by saying where we are now. As of 2017, nearly half of all adolescents age 13-17 were up to date (i.e. had gotten the full number) of shots of the HPV vaccine.
Source: CDC. (2018). National, Regional, State, Selected Local Area Vaccination Coverage Among Adolescents Aged 13-17 Years—United States, 2017. MMRW 67(33)
What percentage of vaccinated youth is the goal?
According to the CDC, “After the quadrivalent HPV vaccine was licensed in 2006, Healthy People 2020 stated an objective of 80% coverage with 3 doses of HPV vaccine for females by age 13 to 15 years. It also stated objectives to “Reduce the death rate from cancer of the uterine cervix below a target of 2.2 deaths/100,000 females (from a baseline of 2.4 per 100,000 in 2007)” and “Reduce invasive uterine cancer to 7.2 new cases per 100,000 females.55 There is also a stated goal to “increase the proportion of women who receive a cervical cancer screening based on the most recent guidelines” with a target of 90% of women 21 to 65 years of age receiving screening (from a baseline of 84.5% in 2008). There are currently no stated goals for reduction of anogenital warts, RRP, or non-cervical HPV-associated cancers.”
What is Healthy People 2020? It’s a program launched by the US Department of Health and Human Services in 2010 that has four overarching goals:
“- Attain high-quality, longer lives free of preventable disease, disability, injury, and premature death;
- Achieve health equity, eliminate disparities, and improve the health of all groups;
- Create social and physical environments that promote good health for all; and
- Promote quality of life, healthy development, and healthy behaviors across all life stages.”
Because it is not looking likely that this goal will be met, the American Cancer Society has set a new goal of 80% coverage with the HPV vaccine for 2026. Note that the Healthy People 2020 goal was specifically set for girls only, whereas the new goal from the ACS is for both girls AND boys. -
20) Is Herd Immunity Possible With The HPV Vaccine?
- The answer is yes!
Herd immunity is a concept where non-immunized individuals are protected against infection by some agent because they are surrounded by a large number of people who have been immunized. These immunized people serve to break a chain of contagion, and as a result the infectious agent does not reach the non-immunized person. The exact percentage of the population that needs to be immunized for the population to be protected varies depending on the ease and mechanism of transmission of the infectious agent. For example, a greater percentage of people need to be immunized to prevent the spread of viruses that are transmitted by coughing or sneezing compared to those like HIV and HPV that are sexually transmitted. Herd immunity becomes very important in protecting those who can’t be immunized for some reason, such as those with weakened immune systems, including newborns, people with HIV, cancer patients who have received chemotherapy and radiation, etc. For sexually transmitted infections (STIs) including HPV, high levels of immunity in one sex induces herd immunity for both sexes in many instances. Vaccinating women against HPV, however, would provide no protection to men who are exclusively homosexual.
A new 17-year study published in JAMA Pediatrics shows that HPV vaccines not only prevent infection in vaccinated individuals but also provide indirect protection to unvaccinated people, demonstrating herd immunity. Conducted in Cincinnati from 2006 to 2023, the research analyzed data from 2,335 adolescent girls and young women, most at higher risk of HPV due to sexual behaviors. Among vaccinated participants, infections caused by HPV types linked to cervical cancer dropped by up to 98.4%, while unvaccinated peers experienced a 71.6% decline, indicating community-wide immunity. The study evaluated three vaccine versions—2-valent, 4-valent, and 9-valent—each covering a broader range of high-risk HPV strains responsible for more than 70% of cervical cancers.
HPV is the most common sexually transmitted infection globally and can lead to cervical, anal, and head and neck cancers. Although most infections clear naturally, persistent high-risk strains account for an estimated 690,000 cancer cases yearly, the majority in women. As vaccination rates in the U.S. have increased to 82% among study participants, infection rates have plummeted, offering strong evidence of the vaccine’s community impact. However, global vaccination coverage remains uneven, with only 31% of girls and 8% of boys receiving at least one dose. Experts emphasize that expanding access to these safe and effective vaccines, along with screening and treatment, could bring the world closer to eliminating cervical cancer.
DeSieghardt, A. et al Population-Level Effectiveness and Herd Protection 17 Years After HPV Vaccine Introduction. JAMA Pediatr. 2025; 10.1001/jamapediatrics.2025.3568
Wikipedia has a very detailed explanation for how herd immunity works.
I also found this interesting visualization graphic that shows how herd immunity provides protection by throwing up barriers around infected people.
Here’s another terrific visualization graphic of herd immunity. It’s set up for measles, but the same principle applies to HPV infections.
————————————————————————————————————————————————————————————————————
Here's some older info for those of you who are interested:
Modeling in this paper suggests that at 80% vaccination coverage of both girls AND boys would lead to the elimination of four strains of HPV, including the two most prevalent cancer causing strains, 16 and 18. M Brisson et al Population-level impact, herd immunity, and elimination after human papillomavirus vaccination: a systematic review and meta-analysis of predictions from transmission-dynamic models. Lancet Public Health. 2016 Nov;1(1):e8-e17. doi: 10.1016/S2468-2667(16)30001-9. Epub 2016 Sep 27.
Even better, here’s a paper with actual data showing the effect of herd immunity with the HPV vaccine in young women in the US that was done 2006-2017. Among women who were vaccinated, 4-valent vaccine–type HPV detection decreased from 35% to 6.7%. Among women who were NOT vaccinated, 4-valent vaccine–type HPV detection decreased from 32.4% to 19.4%.
Spinner C, et al Human Papillomavirus Vaccine Effectiveness and Herd Protection in Young Women. Pediatrics. 2019;143(2):e20181902
This study also provided clear evidence of herd immunity, protecting women who had not yet been vaccinated.
Shahmoradi, Z et al Prevalence of Human Papillomavirus Infection Among Women Born in the 1990s vs the 1980s and Association With HPV Vaccination in the US. JAMA Health Forum. 2022;3(8):e222706. doi:10.1001/jamahealthforum.2022.2706
A landmark Finnish study looked at HPV infection rates in 60,000 girls divided into three groups: unvaccinated; girls-only vaccinated, and both girls and boys vaccinated. The vaccine used was the original Cervarix vaccine, which only targeted two of the most oncogenic strains, 16 and 18. The researchers then followed up with the girls four and eight years after the vaccination to test for 16 different types of genital HPV — HPV 16/18/31/45, the high-oncogenic types, and 12 other types carrying lower cancer risk. In the group with both girls and boys vaccinated, a 50% vaccination coverage per year cohort was sufficient to nearly eliminate the occurrence of the two high-oncogenic HPV types targeted by the vaccine. When the vaccine was just given to girls, the uptake needs to be extremely high (around 90%) to reach the same virus elimination results. By immunizing boys as well the virus has no reservoir to hide in. In addition, HPV45 depletion was observed only in the vaccine group that included boys and girls. No strain depletion was seen in the other two groups. Note that with vaccination protocols in the real world, the percentage of vaccinated who are boys vs girls, and the exact vaccine used (which targeted either two, four, or nine strains of the virus), results may differ from location to location. This may eventually lead to changes to cervical cancer screening protocols since it's believed that nearly all cases of cervical cancer are caused by oncogenic HPV strains. Strain replacement should also occur at the other sites that develop cancer following HPV infection: the back of the throat; the anus, the vagina, the vulva, and the penis.
Because the current vaccine being used targets nine different strains (seven oncogenic, and two that cause genital warts), it's likely that the use of the newer vaccine will speed up the loss of oncogenic strains. One key point: vaccinating both girls and boys greatly accelerates the elimination of the highly oncogenic strains of HPV.
According to this article, “Girls-only vaccination for HPV herd immunity requires 90% of girls to be vaccinated year on year since only half of the population is being protected, but immunizing boys starts to protect the other half of the population and the virus has nowhere to go,” Margaret Stanley, emeritus professor of epithelial biology at the University of Cambridge, who was not involved in the study, wrote in a commentary provided via the Science Media Centre.
At the same time, the samples showed that other HPV types closely related to those targeted by the vaccine had replaced the initial targets. This is not surprising, said Pimenoff: When you have significant variety in a virus type, as with HPV, removing a subset of it leaves a niche that is free to be easily occupied by the remaining strains, which have evolved in a similar way.
Pimenoff, V.N. et al Ecological diversity profiles of non-vaccine-targeted HPVs after gender-based community vaccination efforts. Cell Host & Microbe 31, 1921–1929, November 8, 2023. -
21) What Is The Vaccine Adverse Event Reporting System (VAERS)?
- The Vaccine Adverse Event Reporting System (VAERS) is a reporting process that has been put in place for patients or doctors to record information about problems observed after people have been vaccinated. Its purpose is widely misunderstood. It does NOT exist to track specific and proven adverse reactions caused by vaccines; it is simply there to record information. The purpose of the system is clearly denoted on the VAERS website as follows:
“When evaluating data from VAERS, IT IS IMPORTANT TO NOTE THAT FOR ANY REPORTED EVENT, NO CAUSE-AND-EFFECT RELATIONSHIP HAS BEEN ESTABLISHED. Reports of all possible associations between vaccines and adverse events (possible side effects) are filed in VAERS. Therefore, VAERS COLLECTS DATA ON ANY ADVERSE EVENT FOLLOWING VACCINATION, BE IT COINCIDENTAL OR TRULY CAUSED BY A VACCINE. THE REPORT OF AN ADVERSE EVENT TO VAERS IS NOT DOCUMENTATION THAT A VACCINE CAUSED THE EVENT.”
So the reporting of any event after receiving a vaccination is simply a record. It does NOT prove the vaccine caused that issue. Let me put this in a different context to see if that helps. Imagine if there was a similar system that was in place for people to report problems for some period of time after they have shopped at Target or taken a taxi. That database might note that you began to feel sick four days after your shopping trip, or the taxi ride. But does that mean that your sickness was CAUSED by the shopping excursion or the taxi ride? No. It could be related, but maybe not. Coincidences happen all the time. Keep this in mind as you look at data from VAERS.
If you want to look at specific numbers of claims filed, and those that were paid, and how much the payments were, you can click on this link to get the numbers from the National Vaccine Injury Compensation Program (VICP). They have data from all of the vaccines. Let’s look at HPV for an example and see what the numbers tell us:
Number of doses given (2006-2016): 101,405,935
Total compensable claims filed: 288
Number of claims dismissed: 160
Total compensable claims awarded: 128 (this includes concessions, court decisions, and settlements)
This works out to be 0.00126 percent of those vaccinated against HPV filed a claim and were compensated at some level. Put another way, there was 1 compensated award for every 792,233 doses of vaccine given.
There were an average of 12 claims paid out to those who said they were harmed by the HPV vaccine (again, this court does not require absolute proof to award settlements). “Approximately 70% of all compensation awarded by the VICP comes as result of a negotiated settlement between the parties in which HHS has not concluded, based upon review of the evidence, that the alleged vaccine(s) caused the alleged injury.”
By contrast, 51 people in the US are killed (not just struck) by lightning each year, and sharks attack about 19 people. This illustrates just how safe the HPV vaccine is. Keep in mind that there were a total of 43,371 HPV-associated cancers in 2015 in the US: 24,432 cases in women, and 18,939 cases in men. HPV causes oropharyngeal, anal, penile, cervical, vaginal, and vulvar cancers. It also causes painful genital warts. This is why it’s a good idea to vaccinate both girls AND boys against HPV!
Here’s more data covering ALL vaccines from the US government vaccine injury compensation from the National Vaccine Injury Compensation Program:
“Being awarded compensation for a petition does not necessarily mean that the vaccine caused the alleged injury. In fact:
Attorneys are eligible for reasonable attorneys’ fees, whether or not the petitioner is awarded compensation by the Court, if certain minimal requirements are met. In those circumstances, attorneys are paid by the VICP directly. By statute, attorneys may not charge any other fee, including a contingency fee, for his or her services in representing a petitioner in the VICP.”
“According to the CDC, from 2006 to 2017 over 3.4 billion doses of covered vaccines were distributed in the U.S. For petitions filed in this time period, 6,314 petitions were adjudicated by the Court, and of those 4,328 were compensated. This means for every 1 million doses of vaccine that were distributed, approximately 1 individual was compensated.
Since 1988, over 20,728 petitions have been filed with the VICP. Over that 30-year time period, 17,923 petitions have been adjudicated, with 6,597 of those determined to be compensable, while 11,326 were dismissed. Total compensation paid over the life of the program is approximately $4.1 billion.”
Here’s a good summary look at Why the Government Pays Billions to People Who Claim Injury by Vaccines
Note that Australia has an equivalent database called DAEN: the Database of Adverse Event Notifications. It has the same limitations as VAERS in that the data is self reported, and no evidence of causality can be inferred from the data.
Getting back to the U.S., you should know that payments made to people who allege harm from vaccines are rare. Check out this excellent article Vaccine Injury Claims Are Few and Far Between detailing this story. -
22) What's The Difference Between A Preventative And A Therapeutic Vaccine?
- Most of the time when we speak about HPV vaccines, we are talking about those that are preventative and are used in immunizations to prevent infection with the virus, such as Gardasil 9 (see above). All of the existing vaccines to date have been preventative.
However, efforts are underway to develop therapeutic vaccines, which are designed to be given to patients diagnosed with HPV-caused cancers. These vaccines are often designed to target the E6 and E7 proteins, which are thought to be the key ones the virus uses to turn normal cells into cancer cells. You can read a report about efforts to develop one of these therapeutic vaccines here. As of 2018, there have been no therapeutic HPV vaccines approved in the US by the FDA.
I describe a number of these studies of potentially therapeutic vaccines below:
——————————————————————————————————————————————————————————————————————
From Science Daily: "A new vaccine against cancer-causing human papillomaviruses (HPV) is intended to help increase the rate of HPV vaccinations, particularly in developing countries. Scientists at the German Cancer Research Center (DKFZ) developed a completely new vaccination concept for this purpose. The vaccine is inexpensive and protects mice against almost all cancer-causing HPV types. In addition to preventing new infections, the vaccine also triggers cellular immune responses against HPV-infected cells and may therefore also have a therapeutic effect against existing infections.
In developing their new HPV vaccine, Müller and his colleagues took a systematic approach to solving all these problems. The basis for this was the "predecessor model" PANHPVAX, which was also developed in Müller's laboratory: this exclusively prophylactic vaccine has already proven to be safe in phase I clinical trials and induces protective antibodies against all cancer-causing HPV as well as against some cutaneous papillomaviruses.
For PANHPVAX, the researchers used small fragments of the L2 protein from eight different HPV types. These fragments differ only slightly between different HPV types and can therefore trigger a very broad immune response. To make these protein snippets immunogenic, they were inserted into a suitable scaffold protein derived from a heat-loving microorganism (Pyrococcus furiosus).
"In our current work, we have added a therapeutic component to PANHPVAX, i.e. an antigen that stimulates the cellular immune response," explains Müller. The DKFZ virologists chose the protein E7 of the two high-risk types HVP16 and 18. It is formed very early in the course of an HPV infection in the infected cells and is therefore an ideal target for a cellular immune response to eliminate these cells. However, E7 is also responsible for the malignant transformation of HPV-infected cells. The researchers therefore first had to modify the vaccine antigen so that it no longer posed a threat.
In preclinical studies, the new vaccine cPANHPVAX was able to trigger neutralizing antibodies against all carcinogenic HPV in mice and simultaneously activate cytotoxic T cells against the HPV16 protein E7.
These positive results encouraged the researchers to now produce cPANHPVAX under conditions that comply with Good Manufacturing Practice (GMP) guidelines for pharmaceuticals. The vaccine produced in this way can be used in clinical trials.
"Our major goal is to increase vaccination rates against HPV worldwide, especially in countries with limited resources. Our new, heat-stable vaccine is inexpensive to produce, protects against all cancer-causing HPV types and can potentially neutralize existing infections by combining it with E7." In order to further investigate the promising properties of cPANHPVAX, the researchers are currently developing a concept for clinical testing of the vaccine."
Here's a link to the actual science paper describing this:
Zhao, X. et al A safe and potentiated multi-type HPV L2-E7 nanoparticle vaccine with combined prophylactic and therapeutic activity. npj Vaccines 9, 119 (2024). https://doi.org/10.1038/s41541-024-00914-z.
——————————————————————————————————————————————————————————————————————
An international, drug-company sponsored study has been launched to investigate the use of a therapeutic vaccine in treating CIN2 (this is high grade cervical intraepithelial neoplasia) in women who are contemplating future pregnancies. This therapeutic vaccine, MEDI0457, features two main components. They are VGX-3100, a DNA plasmid containing modified sequences for E6 and E7, and INO-9012, a DNA plasmid containing the immune activator IL-12.The vaccine will be given as an alternative to surgery, which can weaken the cervix and lead to problems in future pregnancies.
——————————————————————————————————————————————————————————————————————
Another therapeutic vaccine being looked at is known as MEL-1, and is also referred to as MVA E2. It is derived from the smallpox virus vaccine MVA, which was originally developed in Germany during the 1940s. The World Health Organization has approved MVA for use in other human vaccines in the early 1990s (note that this does not imply that the U.S. Food and Drug Administration, or FDA, or any other governmental regulatory agency will approve any vaccine based on the use of MVA). Scientists working for Virolab Mexico experimented by inserting certain genes from the Bovine Papillomavirus into MVA. One of the genes inserted was E2, an anti-tumor protein that self-regulates the activity of HVP’s tumor-generating proteins. Why a gene from a cow virus was used instead of the human virus is unclear to me.
In a phase III clinical trial conducted in Mexico, the MVA E2 recombinant vaccinia virus to treat intraepithelial lesions associated with papillomavirus infection. A total of 1176 female and 180 male patients with intraepithelial lesions were studied. They were injected with 107 MVA E2 virus particles directly into their uterus, urethra, vulva, or anus. Patients were monitored by colposcopy and cytology. Immune response was determined by measuring the antibody titer against MVA E2 virus and by analyzing the cytotoxic activity against cancer cells bearing papillomavirus DNA. Papillomavirus was determined by the Hybrid Capture method or by polymerase chain reaction analysis. By histology, 1051 (89.3%) female patients showed complete elimination of lesions after treatment with MVA E2. In 28 (2.4%) female patients, the lesion was reduced to CIN 1. Another 97 (8.3%) female patients presented isolated koilocytes after treatment. In men, all lesions were completely eliminated. All MVA E2–treated patients developed antibodies against the MVA E2 vaccine and generated a specific cytotoxic response against papilloma-transformed cells. Papillomavirus DNA was not detected after treatment in 83% of total patients treated. According to the authors, MVA E2 did not generate any apparent side effects.
Rosales, R. et al. Regression of Human Papillomavirus Intraepithelial Lesions Is Induced by MVA E2 Therapeutic Vaccine. Hum Gene Ther. 2014 Dec 1; 25(12): 1035–1049. Published online 2014 Sep 30. doi: 10.1089/hum.2014.024 FREE paper
Despite these apparently promising results, I have been unable to find any info regarding licensing of this vaccine by the FDA.
——————————————————————————————————————————————————————————————————————
There is a similar sounding, but clearly distinct trial currently in progress at multiple locations in the U.S. NCT03610581. Safety, Reactogenicity and Immunogenicity of Adenovirus Serotype 26 (Ad26)- and Modified Vaccinia Ankara (MVA)-Vectored Vaccine Components in Otherwise Healthy Women With Persistent Human Papillomavirus HPV16 or HPV18 Infection of the Cervix. It is sponsored by Janssen Vaccines & Prevention B.V. According to the clinical trials.gov website, “Participants will receive a dose of adenovirus serotype 26 (Ad26)-human papillomavirus (HPV)16 or HPV18 (Ad26.HPV16 or Ad26.HPV18) as prime immunization and a dose of Modified Vaccinia Ankara (MVA)-HPV16/18 (MVA.HPV16/18) as boost immunization.” This is clearly different from the Mexican trial cited above. The trial started in 2018.
So what, exactly, are these vectors? According to the paper below, the investigators “developed HPV16- and HPV18-specific antigens consisting of fusion proteins of E2, E6 and E7. The vaccine will be suitable for every disease stage, from incident and persistent infections where E2 is predominantly expressed up to late stages where E6 and E7 expression are upregulated. Importantly E6 and E7 are pre- sent as reordered fragments to abrogate the transforming activity of these two proteins.”
Khan, S. et al. Development of a replication-deficient adenoviral vector-based vaccine candidate for the interception of HPV16- and HPV18-induced infections and disease. Int. J. Cancer: 141, 393–404 (2017) FREE paper.
——————————————————————————————————————————————————————————————————————
Another therapeutic vaccine approach is being tested in cervical intraepithelial neoplasia grades 2 and 3 using a drug known as Tipapkinogen Sovacivec therapeutic HPV vaccine. You can read about it here. Early results from a randomized controlled phase II trial with 2.5 years of follow-up look promising. The drug completely resolved CIN 3 lesions significantly more frequently than placebo; completely cleared HPV16 viral DNA associated with CIN 2/3 significantly more often than placebo; achieved significantly greater complete resolution rates of CIN 2/3 regardless of HR HPV type; and offered 36% complete resolution or partial response of CIN2/3 associated with all HR HPV types.
What is Tipapkinogen Sovacivec (also referred to here as TS)? According to the paper below, it is a “modified vaccinia virus Ankara (MVA) is a highly attenuated replication-deficient strain of vaccinia virus used widely as a gene- delivery system of vaccines. TS has inserted genes that code for three proteins: human cytokine IL-2, and modified forms of HPV 16 E6 and E7 proteins that have been rendered non oncogenic. MVA by itself contributes to the immune reaction by the induction of an Interferon-alpha response [11]. Upon sub-cutaneous injection, TS infects the surrounding cells. The expressed HPV16 E6 and E7 proteins are then processed and presented by dendritic cells which are co-activated by the viral infection. These dendritic cells migrate to the draining lymph-node and present E6 and E7 peptides to the naive T-cells present in the lymph-node, which should allow development of a targeted cell mediated immune response.”
Harper, D.M. et al The efficacy and safety of Tipapkinogen Sovacivec therapeutic HPV vaccine in cervical intraepithelial neoplasia grades 2 and 3: Randomized controlled phase II trial with 2.5 years of follow-up. Gynecologic Oncology. 2019
You can find the paper for FREE here, or read this article about how this treatment is being tested at the U. of Michigan.
——————————————————————————————————————————————————————————————————————
Another approach seeks to make a therapeutic vaccine by expressing fragments of the E2, E6, and E7 proteins in and adenovirus vector. By using just fragments it prevents the proteins from having a cancer-promoting function while creating immunogenic targets for training the immune system. Here’s a brief summary:
“High-risk Human papilloma virus (HPV) types are the causative agents of cervical cancer and several other anogenital malignancies. The viral proteins expressed in the (pre)malignant cells are considered ideal targets for immunological intervention. Many approaches have been evaluated for this purpose, mostly aiming at the induction of HPV16 E7- and/or E6-specific cellular immunogenicity. As clinical success has so far been limited, novel approaches are required. We describe the development and pre-clinical testing of a vaccine candidate consisting of replication-deficient adenovirus type 26 and 35 based vectors for the interception of HPV16- and HPV18-related disease. We developed HPV16- and HPV18-specific antigens consisting of fusion proteins of E2, E6 and E7. The vaccine will be suitable for every disease stage, from incident and persistent infections where E2 is predominantly expressed up to late stages where E6 and E7 expression are upregulated. Importantly E6 and E7 are pre- sent as reordered fragments to abrogate the transforming activity of these two proteins. Loss of transforming activity was demonstrated in different in vitro models. Robust T-cell immunogenicity was induced upon immunization of mice with the vaccine candidate. Finally, the developed vaccine vectors showed considerable therapeutic efficacy in the TC-1 mouse model. The absence of transforming activity of the antigens and the favorable immunogenicity profile of the adenovirus based vectors along with the fact that these vectors can be readily produced on a large scale makes this approach attractive for clinical evaluation.”
Khan et al Development of a replication-deficient adenoviral vector-based vaccine candidate for the interception of HPV16- and HPV18-induced infections and disease. Int. J. Cancer: 141, 393–404 (2017) FREE download
——————————————————————————————————————————————————————————————————————
Another approach seeks to make a therapeutic vaccine against HPV by injecting long peptide fragments of the E6 and E7 proteins of HPV, which are thought to be the primary viral proteins involved in causing cancer. The investigators looked at the immunogenicity and efficacy of their therapeutic vaccine in women with HPV-16–positive, high-grade vulvar intraepithelial neoplasia. “Twenty women with HPV-16–positive, grade 3 vulvar intraepithelial neoplasia were vaccinated three or four times with a mix of long peptides from the HPV-16 viral oncoproteins E6 and E7 in incomplete Freund's adjuvant. The end points were clinical and HPV-16–specific T-cell responses. The most common adverse events were local swelling in 100% of the patients and fever in 64% of the patients; none of these events exceeded grade 2. At 3 months after the last vaccination, 12 of 20 patients (60%; 95% confidence interval [CI], 36 to 81) had clinical responses and reported relief of symptoms. Five women had complete regression of the lesions, and HPV-16 was no longer detectable in four of them. At 12 months of follow-up, 15 of 19 patients had clinical responses (79%; 95% CI, 54 to 94), with a complete response in 9 of 19 patients (47%; 95% CI, 24 to 71). The complete-response rate was maintained at 24 months of follow-up. All patients had vaccine-induced T-cell responses, and post hoc analyses suggested that patients with a complete response at 3 months had a significantly stronger interferon-γ–associated proliferative CD4+ T-cell response and a broad response of CD8+ interferon-γ T cells than did patients without a complete response.” The authors concluded that “clinical responses in women with HPV-16–positive, grade 3 vulvar intraepithelial neoplasia can be achieved by vaccination with a synthetic long-peptide vaccine against the HPV-16 oncoproteins E6 and E7. Complete responses appear to be correlated with induction of HPV-16–specific immunity.”
Kenter, G.G. et al Vaccination against HPV-16 Oncoproteins for Vulvar Intraepithelial Neoplasia. N Engl J Med 2009; 361:1838-1847
DOI: 10.1056/NEJMoa0810097. FREE download
——————————————————————————————————————————————————————————————————————
Another approach seeks to make a therapeutic vaccine against HPV by creating a multi-genotype immunogen that comprises segments from each of six early proteins and is delivered by replication-deficient chimpanzee adenovirus and MVA vectors. This immunogen is predicted to provide coverage of 85% of circulating global cancer-causing HPV genotypes that cause cervical cancer, and builds upon existing concepts that have been focusing predominantly on E6/E7 from HPV16/18. This particular vaccine is designed to elicit an immune response against six different HPV encoded proteins, not just E6 and E7 as some of the other vaccines do.
A trial of this vaccine is planned to begin in March, 2020 and is an international undertaking. It is expected to involve 15 hospitals in the UK and Belgium. The doctors hope to recruit 105 women aged 25 to 55 with a persistent high-risk HPV infection. While 73 will be given two shots of a particular dose of the vaccine, the rest receive a placebo. They will then be tested for the presence of HPV over a period of 12 months to see if the virus has disappeared.
The team hopes to recruit 105 women aged 25 to 55 with a persistent high-risk HPV infection. While 73 will be given two shots of a particular dose of the vaccine, the rest receive a placebo. They will then be tested for the presence of HPV over a period of 12 months. Women interested in joining the trial can contact the team via email at hpv-study@wrh.ox.ac.uk
Hancock, et al. A multi-genotype therapeutic human papillomavirus vaccine elicits potent t cell responses to conserved regions of early proteins. Scientific Reports (2019) 9:18713 | https://doi.org/10.1038/s41598-019-55014-z FREE download
——————————————————————————————————————————————————————————————————————
Another approach seeks to make a therapeutic vaccine against HPV by using a mix of long peptides from the HPV-16 viral oncoproteins E6 and E7 in incomplete Freund's adjuvant. The study was done in women diagnosed with vulvar intraepithelial neoplasia. In view of the low rate of spontaneous regression of lesions in patients with grade 3 vulvar intraepithelial neoplasia, a single-center, single-group (noncontrolled), observational phase 2 study was designed. The investigators concluded that vaccination with synthetic long peptides that represent the entire length of the two oncoproteins E6 and E7 of HPV-16 is effective over a period of 12 to 24 months for the treatment of high-grade vulvar intraepithelial neoplasia lesions. This clinical effcacy is probably related to a vaccine- induced HPV-16–specific T-cell response. This study was conducted by the Leiden University Medical Center (LUMC), which holds a patent on the use of synthetic long peptides as vaccine (U.S. patent number 7,202,034). The LUMC does not share the financial benefit from this patent with its employees. ISA Pharmaceuticals, a biotechnology company, has licensed the patent from the LUMC.
Kenter et al Vaccination against HPV-16 Oncoproteins for Vulvar Intraepithelial Neoplasia. N Engl J Med 2009; 361:1838-1847 DOI: 10.1056/NEJMoa0810097. Note: as this study was done in 2009, it is unclear what happened next.
——————————————————————————————————————————————————————————————————————
IMV Inc. is testing a therapeutic vaccine against E7, which is one of two viral HPV proteins expressed in cervical and other HPV-related cancers. The hope is that the DPX-E7 HPV vaccine may stimulate the human immune system to mount an anti-cancer T cell response against tumors expressing the HPV16 E7 protein. Trials are focused on patients with incurable oropharyngeal, cervical and anal cancers caused by HPV. ClinicalTrials.gov Identifier: NCT02865135 -
23) Does HPV Vaccine Coverage Vary From State To State?
- In the US, vaccination rates vary quite a bit between the states. They also, of course, vary a lot over smaller areas within each state, and at least some of that is driven by pockets of anti-vaccine parents. For example, in the Seattle area where I live, there’s a community on Vashon Island that has had vaccination opt-out rates that are five times the state average. However, due to a recent measles outbreak in Vancouver, WA, it’s been reported that vaccination rates even on Vashon Island have soared in response to this.
So what are the laws covering vaccination? According to the Kaiser Family Foundation, “Presently at least 25 states and Washington D.C. have laws that either require HPV vaccination for school entry, provide funding to cover the costs of the vaccines, or support public education about HPV and the vaccine. D.C. and Virginia require the vaccine for girls to enter the sixth grade, but allow parents to opt out of the requirement due to medical, moral, or religious opposition. Rhode Island requires ALL seventh-grade students to be vaccinated.” In 2020, Hawaii became the next state to require HPV vaccination of all students entering the sixth grade. in 2021 Virginia will require children entering the 7th grade to have completed a series of two or three doses of HPV vaccines. A parent or guardian has the right to decide if their child receives the HPV vaccine with no requirement for a medical or religious exemption.
You can see a map with state by state vaccination rates below. Rural states in general have much lower vaccination rates that other states. This graphic nicely illustrates the more than two-fold variation in HPV vaccination rates across all 50 states. 2019 data.
If you're interested in exploring the various factors that account for the large differences in HPV vaccination in the state with the highest rate (Rhode Island) and the lowest rate (Mississippi), check out this blog post from the Journal of Clinical Pathways by Logan, K. et al (2024): A Tale of Two States: Examining the Best and Worst Performing States for HPV Vaccination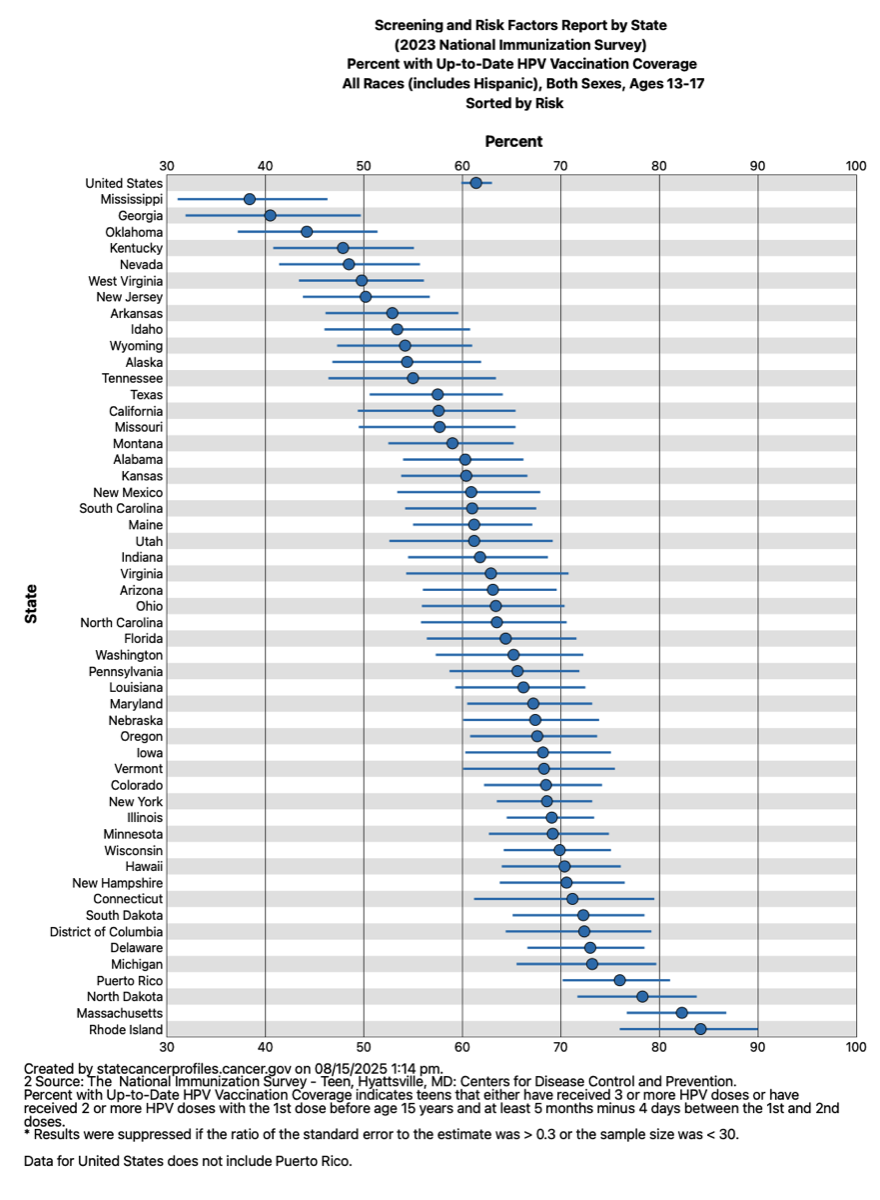 The CDC had set a goal, as part of the Healthy People 2020 initiative, of getting to 80% vaccination rates for girls by 2020. As we are unlikely to meet this goal, the American Cancer Society has put forth a new goal of 80% vaccination rate for both girls AND boys by 2026.
The CDC had set a goal, as part of the Healthy People 2020 initiative, of getting to 80% vaccination rates for girls by 2020. As we are unlikely to meet this goal, the American Cancer Society has put forth a new goal of 80% vaccination rate for both girls AND boys by 2026.
You can also look at this paper published in the journal Pediatrics, Legislation to Increase Uptake of HPV Vaccination and Adolescent Sexual Behaviors. The authors concluded, “Implementation of HPV legislation was not associated with changes in adolescent sexual behaviors in the United States.”
The latest numbers in 2019 of the number of adolescents fully vaccinated against HPV (i.e. they have had all of their required doses) ranged from about 47 to 57%, depending on whether or not they lived in a metropolitan area, and their economic status. Elam-Evans, L.D. et al. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13–17 Years — United States, 2019. CDC MMWR Weekly / August 21, 2020 / 69(33);1109–1116. FREE download.
A number of studies have been done to try and figure out the best way to raise HPV vaccine immunization rates. These include reminder phone calls to parents; having HPV vaccines available in schools, and getting clinics to make sure and recommend the vaccine. All of these interventions are considered cost effective. See Spencer, J.C. et al Cost-effectiveness of Interventions to Increase HPV Vaccine Uptake. Pediatrics November 2020, e20200395; DOI: https://doi.org/10.1542/peds.2020-0395
Another promising approach: pass laws that enable adolescents to get the vaccine without their parents consent. I a 2021 study, researchers analyzed adolescent vaccination data in the United States from 2015 to 2018, comparing HPV vaccination rates between those jurisdictions that allow this with those who don’t. The data set included 81,889 adolescents aged 13 to 17. They found a positive correlation between those jurisdictions that allowed adolescents to get the HPV vaccine on their own and higher first-dose vaccination rates. In places where these laws are in effect, 67.9% of adolescents had received at least the first dose of the vaccine compared with 61.4% of adolescents in states without the laws.
Torres, A.R. et al. State Laws Permitting Adolescent Consent to Human Papillomavirus Vaccination and Rates of Immunization. JAMA Pediatrics doi:10.1001/jamapediatrics.2021.4591
A good resource for pediatricians is Let’s Talk Vaccines: A Clinician’s Guide to Addressing Vaccine Hesitancy and Saving Lives by Gretchen LaSalle (2020). It’s a guide for doctors that was written to teach them about vaccines, and to advise them on current best practices to convince parents who are hesitant to vaccinate their kids to actually do so. Written by a family doctor, it’s primary goal is to educate clinicians about the anti-vaccine movement, and to provide them with tools that can be used to convince parents that vaccines really are safe, effective, and will protect their children from dangerous diseases.
A survey of parents in the US published in Feb. 2021 revealed that 60% of them had NO INTENTION of vaccinating their kids with the HPV vaccine despite a recommendation from their healthcare provider.
Sonawane, K. et al. HPV Vaccine Recommendations and Parental Intent. Pediatrics February 2021, e2020026286; DOI: https://doi.org/10.1542/peds.2020-026286. -
24) Do All Major Religions Approve Of The HPV Vaccine?
- Yes they do. The short answer is that ALL of the major religions of the world are OK with ALL of the currently available vaccines. Here’s a pretty comprehensive review of the subject:
Grabenstein, J. What the World’s religions teach, applied to vaccines and immune globulins. Vaccine 31 (2013) 2011–2023. FREE download.
Note that the courts in the US have consistently ruled against religious objections raised by parents who don’t want to vaccinate their children. Here’s an article discussing a recent case where the court ruled against the parents. One court ruling said that “the right to practice religion freely does not include liberty to expose the community or the child to the communicable disease or the latter to ill health or death.” People v. Pierson, 176 N.Y. 201, 68 N.E. 243.
Despite the fact that none of the world’s religions are opposed to vaccines, some religious schools in New Zealand are refusing to participate in government funded in-school vaccinations with the HPV vaccine. Most of these schools had a Christian religious background, and this ties into misinformation campaigns that the HPV vaccine somehow leads to teenage promiscuity. Study after study have debunked this myth.
Source: Some religious schools refusing to offer HPV vaccine. See FAQs 34 and 35 below for more details. -
25) Who Invented The HPV Vaccine?
- The vaccine was first developed at the University of Queensland in Australia by researchers Ian Frazer and Jian Zhou. Their work built upon the initial discovery that HPV was associated with and causes cervical cancer, which is credited to German researcher Harald zur Hausen. He shared the Nobel Prize in Medicine in 2008 for this groundbreaking work, along with the discoverers of the HIV virus.
Professor Frazier spent time in recent years spearheading an effort to develop a therapeutic vaccine that can be used as an immuno-therapeutic approach to treat those with HPV-caused oropharyngeal cancers. He retired from his research duties in Nov. 2022.
In 2024 Drug Discovery News published a nice concise history of the development of the vaccine. You can view it here. -
26) What Ingredients Are In The HPV Vaccine?
- The current Gardasil 9 HPV vaccine contains the follow substances: amorphous aluminum hydroxyphosphate sulfate (AAHS), sodium chloride, L-histidine, polysorbate 80, sodium borate, and yeast protein.
These adjuvants and excipients are substances added to vaccines that serve two purposes: to stabilize the vaccine, and to make the vaccine more effective.
Of the ingredients:
Yeast protein represents an engineered form of the L1 protein made by nine different strains of HPV. These self-assemble into structures known as virus-like particles (VLPs). They are actually manufactured in yeast cells via genetic engineering, and then are highly purified. These VLPs form the core component of the vaccine. If you have an allergy to yeast, ask your doctor if getting the HPV vaccine is right for you.
AAHS is the adjuvant that makes it work better. The L1 proteins adhere to the aluminum salts, and makes it easier for our immune system to recognize these proteins and develop an immune response.
Sodium chloride (salt), L-histidine, polysorbate 80, and sodium borate are there to stabilize the vaccine so that it does not degrade over time. Vaccines need to be stored cold so that they do not degrade.
The CDC has a very clear explanation of what adjuvants are:
“An adjuvant is an ingredient used in some vaccines that helps create a stronger immune response in people receiving the vaccine. In other words, adjuvants help vaccines work better. Some vaccines that are made from weakened or killed germs contain naturally occurring adjuvants and help the body produce a strong protective immune response. However, most vaccines developed today include just small components of germs, such as their proteins, rather than the entire virus or bacteria. Adjuvants help the body to produce an immune response strong enough to protect the person from the disease he or she is being vaccinated against. Adjuvanted vaccines can cause more local reactions (such as redness, swelling, and pain at the injection site) and more systemic reactions (such as fever, chills and body aches) than non-adjuvanted vaccines.”
The current vaccine against HPV, Gardasil 9, is not a weakened virus vaccine. It contains but a single protein made by the virus (see the answer to question 27 above). That’s why an adjuvant is used to generate a stronger immune response. In the case of Gardasil 9, this adjuvant is an aluminum based compound. Aluminum based adjuvants are the most commonly used ones in vaccines. The CDC notes that “aluminum salts, such as aluminum hydroxide, aluminum phosphate, and aluminum potassium sulfate have been used safely in vaccines for more than 70 years. Aluminum salts were initially used in the 1930s, 1940s, and 1950s with diphtheria and tetanus vaccines after it was found they strengthened the body’s immune response to these vaccines.”
To learn even more about the levels of aluminum in vaccines vs. the levels found in breast milk and formula, and why aluminum amounts in vaccines are too small to be harmful, check out this detailed Q&A from the Vaccine Information Center at the Children’s Hospital of Philadelphia.
You can also look at this page on vaxplanations to see a good explanation about why aluminum in vaccines is not a safety risk, or at this page produced by the Immunization Advisory Centre of New Zealand. -
27) How Do The HPV And Shingles Vaccines Work Differently?
- The short answer is that the two viruses are of different types and function in distinct ways to cause disease. Human papilloma virus infections are generally fought off by your immune system, but in some cases the virus itself integrates itself into your cellular DNA. On rare occasions this leads to the development of cancer, sometimes many decades later. Put another way, it’s not an active viral infection that causes disease; its the activity of only a few viral genes within your cells that can eventually lead to problems. The vaccine is meant to attack the virus BEFORE it can integrate itself into your DNA. The vaccine cannot prevent the cells from developing cancer once the viral DNA has been integrated, nor does it target the infected cancer cells.
With the chickenpox virus (varicella-zoster) that causes shingles, the entire virus itself can lurk for decades within your nerve cells. As you get older, a decline in the efficiency of your immune system allows the virus to re-emerge, where it can lead to the painful rashes and nerve damage associated with shingles. The shingles vaccine works by generating an immune response against the entire virus, thereby preventing it from causing disease, or at least lessening severity.
The incidence of infection with HPV and chickenpox viruses are similar in that the infection rate is very high in adults in the U.S. More than 90 percent of sexually active adults will get an HPV infection during their lifetimes, and nearly 100 percent of adults will have been exposed to the chickenpox virus (even if they don’t realize it). Gardasil 9 (the current HPV vaccine) is targeted at preventing cancer and genital warts in older adults (except for cervical cancer, which strikes younger women), and the shingles vaccine (Shingrix) is also targeted at the older adult population. In that way they share another similarity. However, the HPV vaccines are meant to be given to kids (and now adults up to age 26), whereas Shingrix is only given to older adults in their 50s, 60s, and older.
The viruses are transmitted in different ways. Chickenpox is transmitted from person to person by directly touching the blisters, saliva or mucus of an infected person. It can also be transmitted through the air by coughing and sneezing. In contrast, HPV is passed via sexual contact; it is NOT transmitted via coughing and sneezing. See question 4 on the HPV FAQ page for more details.
Finally, researchers are trying to develop therapeutic vaccines against HPV that would work after you’ve been infected, just as the shingles vaccine works following infection. Whether such efforts will be successful is unknown. See the answer to FAQ 23 above for more details. -
28) Are There New HPV Vaccines Coming?
- GSK, which makes the Cervarix HPV vaccine, has entered into a collaboration agreement with collaborative agreement with the Chinese company Xiamen Innovax Biotech to develop and commercialize a next generation HPV vaccine. The partnership will aim to deliver a HPV vaccine that uses GSK’s adjuvant systems that is part of the Cervarix vaccine. Innovax has already developed a cervical cancer vaccine, Cecolin, which is HPV 16 & 18 bivalent – these two HPV types are known to cause at least 70% of cervical cancers. This GSK/Innovax vaccine was approved for sale in China on Dec. 31, 2019. Innovax also has a 9-valent HPV vaccine in a phase 2 clinical trial, which will help to protect individuals against diseases caused by nine types of HPV. Note that the GSK/Innovax vaccine uses a different adjuvant system than Merck’s Gardasil 9. The adjuvant is GSK's proprietary AS04 adjuvant system. AS04 is composed of an aluminium salt and monophosphoryl lipid A (MPL); MPL is an immunostimulant capable of directly activating key immune mechanisms, which will ultimately enhance the immune response to the antigens included in the vaccine.
It was announced in late March 2020 that China's first domestically produced vaccine against the human papillomavirus (HPV), Cecolin, will be available by appointment from May, making China the third country in the world to achieve an independent HPV vaccine supply after the US and the UK. Prior to the new vaccine, HPV vaccines available in China were all imported ones, produced by a British pharmaceutical company, which makes a two-valent HPV vaccine and a US drugmaker that produces a four-valent vaccine and a nine-valent HPV vaccine, according to a December notice published on the official website of the National Medical Products Administration.
“The vaccines, especially the 9-valent one, have been in short supply in China, compared to the high demand. Statistics show that a total of 1.46 million doses of HPV vaccines were issued in China in 2017; 7 million issued in 2018; and 8.7 million issued from January to November in 2019. But there are currently 356 million people aged from 9 to 45 in China who are potential candidates for HPV vaccination, according to media reports.
A staff member at a health service center in Jing'an district of Shanghai told the Global Times on Tuesday that people now need to wait about two to three months to get four-valent and nine-valent vaccines at their center.
"I registered for vaccination with the four-valent HPV vaccine at the health service center of my community in October last year and have not been vaccinated yet," Zhang Yanli, a Shanghai resident, confirmed with the Global Times.
The new vaccine is much cheaper with each dose priced at 329 yuan ($46.50), compared to imported ones.
The staff member at the Jing'an service center said that vaccination with the all three types of imported vaccines take three doses. The two-valent and four-valent vaccines at the center cost 585.5 yuan and 808.5 yuan per dose respectively, while the nine-valent one could reach over 1,300 yuan per dose.
The price is even higher at private clinics. At a Shanghai-based private clinic that Global Times reached out to, three doses of imported two-valent HPV vaccines cost 2,788 yuan, the four-valent costs 3,888 yuan and the nine-valent costs 5,980 yuan.
"I am going to get vaccinated (with the domestically made vaccine), it is much cheaper," one Sina Weibo user commented, while some others are still looking forward to four- or nine-valent ones to be developed in China.
Wang Jun (pseudonym), a Beijing based medical expert in immunology, sees the new vaccine as a sign of China's huge market in HPV vaccine and expects to see China-made HPV vaccines that cover more virus types. "Chinese women have high regard for HPV vaccines as people are more likely to be protected through one immunization," Wang added.
A nine-valent vaccine by the company has reportedly entered into a clinical trial.”
——————————————————————————————————————————————————————————————————————
One new approach is to make the HPV vaccines not against the L1 protein, but against the L2 protein of the virus. The idea behind this is to develop a vaccine that effectively protects against many more dangerous strains of HPV than the nine strains (seven of which cause cancer) that are protected against by Gardasil 9. Here’s a pretty good look at this approach:
L2-Based Human Papilloma Virus Vaccines: Current Status and Potential
——————————————————————————————————————————————————————————————————————
Another new approach is to make the HPV vaccine in plants. Why would people want to do that? Simply because it might be cheaper to produce. Making vaccine components in plants would be a way to get the cost of the vaccine down, which would make it easier to get it to more people worldwide. It might also make it easier to create a vaccine that guards against more strains of the virus than the current standard, Gardasil 9, which only protects against nine strains. In this study, they expressed the L2 protein encoded by HPV, whereas the current vaccine targets the L1 protein (see above about the L2 protein). The resulting proteins were shown to be highly immunogenic in mice.
This is simply a demonstration project for the technology. You can read about this project here, or look at the scientific paper reporting it:
Diamos et al Vaccine synergy with virus-like particle and immune complex platforms for delivery of human papillomavirus L2 antigen. Vaccine Volume 37, Issue 1, 3 January 2019, Pages 137-144. (FREE download).
——————————————————————————————————————————————————————————————————————
Another approach that’s being investigated is using lactic acid producing bacteria that produce genetically engineered parts of proteins encoded by HPV to protect women from developing cervical cancer. No injections would be required in this approach. Bacteria that normally colonize the vagina would be modified and given to women; these bacteria would induce an immune response to the HPV proteins, allowing women to eliminate the virus if they get infected. Details below:
Taghinezhad‐S, S. et al. Twenty years of research on HPV vaccines based on genetically modi ed lactic acid bacteria: an overview on the gut‐vagina axis. Cellular and Molecular Life Sciences 2020; https://doi.org/10.1007/s00018-020-03652-2 ) (FREE download) -
29) Can You Get The HPV Vaccine From Your Dentist?
- Yes, and no. Oregon just became (May 2019) the first state in the country that will allow dentists to give all vaccines to their patients. Minnesota and Illinois also allow dentists to administer vaccines, but only to protect against the flu and only in adult patients. While it’s unlikely that many people will turn to their dentists for their MMR, chickenpox, or shingles vaccines, this new law provides dentists an opportunity to both educate and administer the HPV vaccine to their patients. There’s a good rationale for this: HPV causes about 70 percent of oropharyngeal cancers in both men and women. The vaccine, if given to people prior to infection, will prevent the majority of these cancers from every happening.
Oregon is, however, the only state that allows dentists to vaccinate. Now that they have blazed this trail, other states may follow their lead. Many states will likely look to Oregon in a few years to see how successful this program has been statewide.
There are some headwinds that need to be overcome for dentists to become frequent providers of vaccines:
1) Education of dentists about the advantages of providing vaccines to their patients. The Oregon Health Sciences University is working with the Oregon Board of Dentistry, Oregon Board of Pharmacy, Oregon Health Authority, and the Oregon Dental Association to determine how dentists should be trained to provide vaccinations. As the state’s only dental school, the School of Dentistry will likely provide hands-on vaccination training to both practicing dentists and dental students. Which vaccines should dentists give? Since HPV causes a large percentage of oropharyngeal cancers in both men and women, it would make sense for dentists to offer to vaccinate their patients to prevent this. Dentists need to be educated about the fact that HPV causes this type of cancer, and what they can do about it. It’s likely that dentists will generally focus on giving only a subset of possible vaccines rather than give them all. It doesn’t make sense, for example, for them to give vaccines that traditionally are given to babies to older kids. In the case of HPV, dentists can also help with oral cancer exams and sending patients that have any suspicious findings to see an ENT doctor. Dentists could be in the unique position of both preventing the oral cancers caused by HPV as well as helping to screen older patients for the presence of HPV-caused cancers.
2) Educate parents as well. Patients are not used to getting vaccines from dentists, only from their doctors. They will need to be made more comfortable with this new way of doing things.
3) A need to set up their offices for vaccinations. This will require dentists to purchase special refrigerators that can store vaccines at the proper temperature, and that keep a record of that. Dentists will also likely want to subscribe to electronic health records (EHR) that will record the vaccination information and interface with similar EHR systems used by doctors. This is to avoid having individuals vaccinated against the same diseases by both their doctors and their dentists because the patients themselves do not always remember when or if they got particular vaccines, or who gave it to them.
4) Insurance coverage will be important here. Dentists will need to coordinate with different insurance providers (e.g. medical insurance) to provider reimbursement for vaccines, or dental insurers will need to start providing vaccine coverage as well. -
30) What's The Focus Of TV Ads For The HPV Vaccine?
- The early ads for the first HPV vaccine (Cervarix) were focused exclusively on vaccinating girls, and the intent was clearly on prevention of cervical cancer.
That’s changed now with current ad campaigns making the case that girls AND boys need to be vaccinated. The only HPV vaccine still being used in the US is Gardasil 9 that’s produced by Merck. They’ve run several types of ad campaigns as of late. The focus of the first campaign was on showing parents feeling guilty that they didn’t vaccinate their kids, who went on to develop HPV-caused cancers. Here’s an example.
The second ad campaign by Merck is called Versed, and focuses on reaching out to young millennials with an educational question and answer approach. Some liked the approach, but I question how effective it will be on a population that has had all of their vaccination decisions made by their parents when they were growing up.
A new ad campaign was launched in 2020 called Not My Child. The focus once again is on cancer prevention, with parents telling the camera that HPV is “not welcome” and to “get back”. A more threatening vibe than in some of their earlier TV spots. You can find an example here.
In 2021 Merck started running ads for their Gardasil 9 HPV vaccine targeting adults age 27 to 45. This is their first effort to target adults and it comes after the FDA raised the top age limit for getting the vaccine from 26 to 45. Here’s one of their “Help Protect Yourself” commercials. -
31) How Many Strains Are There Of HPV? How Many Cause Cancer?
- Lots. Scientists have found around over 170 different strains of HPV. The strains are not equally prevalent in people. Some are quite common, while others are very rare. Only strains that either cause cancer or genital warts are targeted by the current vaccine.
There are 16 strains that are thought to cause cancer (16, 18, 31, 33, 34, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68 and 70). These strains are often referred to as “high risk” strains. The term 'high-risk' means that these types of HPV are more likely than other types to cause cancer. However, most HPV-associated cancers are linked to just two types of HPV: types 16 and 18. There are over 170 different types of HPV that have been identified to date. Forty HPV strains are sexually transmitted.
The current HPV vaccine, Gardasil 9, provides protection against seven of these strains: 16, 18, 31, 33, 45, 52, and 58. -
32) Can Minors Get The HPV Vaccine Without Parental Consent?
- Sometimes. It depends on where they live.
According to this 2019 report from NBC News, each state has legal exceptions that allow minors to get diagnosed and treated for sexually transmitted diseases. In addition to New York, California, Delaware and Washington, D.C., allow teens under 18 to be vaccinated for HPV and hepatitis B, which is also sexually transmitted.
There are at least 24 states that allow dependent teens to be vaccinated without their parents’ consent. Generally, unless teens are legally emancipated, married or are already parents, they have no recourse when their parents or other legal guardians refuse vaccines, including the HPV shot, on their behalf.
However, because of the rise of anti-vaccination movement and concern over the measles outbreaks in the U.S., more state legislatures are trying to create a legal way for dependent teens to get vaccinated, in particular for HPV, without their parents' consent. Difficulties in achieving this legislatively have led some state Departments of Health (e.g. NY state) to change regulations allowing teenagers to get the HPV vaccine on their own.
Expect this topic to be in flux for the next few years, and results will vary from state to state. HPV vaccination coverage continues to lag well behind the national goal of 80% series completion, and is well behind other vaccinations. There are a number of attitudinal, behavioral, and access barriers that prevent robust uptake of this life-saving vaccine. One way to increase the vaccination rate would be to permit adolescents to consent to HPV vaccination for themselves. Unfortunately, there are legal hurdles to be overcome in many states. Even in areas where self-consent is legal, there can still be barriers due to lack of awareness of the policy among healthcare providers and adolescents. Other barriers to implementation of self-consent include resistance from anti-vaccine misinformation campaigns, and parent rights activists, the reluctance of providers to agree to vaccinate even in areas where self-consent is legally supported, and threats to patient confidentiality.
See Zimet, G.D. et al Adolescent Consent for Human Papillomavirus Vaccine: Ethical, Legal, and Practical Considerations. J Pediatr. 2021 Apr;231:24-30. doi: 10.1016/j.jpeds.2021.01.026. Epub 2021 Jan 20.
Also see Chido-Amajuoyi, O.G. et al Safety Concerns or Adverse Effects as the Main Reason for Human Papillomavirus Vaccine Refusal. National Immunization Survey–Teen, 2008 to 2019. JAMA Pediatr. Published online June 28, 2021. doi:10.1001/jamapediatrics.2021.1585 FREE Download -
33) If HPV Is So Dangerous, Why Don't More Parens Vaccinate Their Kids?
- This is a very complex subject that’s been looked at in a number of studies. There are many reasons, and they cut across all parts of the ideological spectrum. Many parents are simply uninformed about the long-term dangers of HPV infections, and don’t understand the need to vaccinate boys as well as girls. They’ve picked up on the general climate of fear and misinformation about vaccines that pervades some communities. This leads them to take the path of least resistance and skip the vaccines.
Across Europe anti-vaccine folks focus a lot of attention on the HPV vaccine: Inside the anti-vaccine campaign that targets young women. They try to scare parents by telling them that the vaccine will make their daughters promiscuous (although there is no data to support this assertion, and plenty of data contradicting it; see FAQ 35 below).
Parents also grossly underestimate the age at which kids start to have sex, and the percentage of them that do. As you can see in the graphic below, 20% of kids are having sex before the age of 15! The data below are from the CDC and can more details can be found here.
You can also find out more about the ages at which men and women become sexually active all around the world in the following two articles:
Ann Burchell. Sexual behavior and population transmission of HPV.
Wellings, K. Sexual behaviour in context: a global perspective. The Lancet. 368, issue 9548, 1706-1728, 2006. FREE Download
Sadly, a survey of parents in the US published in Feb. 2021 revealed that 60% of them had NO INTENTION of vaccinating their kids with the HPV vaccine despite a recommendation from their healthcare provider.
Sonawane, K. et al. HPV Vaccine Recommendations and Parental Intent. Pediatrics February 2021, e2020026286; DOI: https://doi.org/10.1542/peds.2020-026286.Let’s take a look at many of the oft-stated (but erroneous) reasons parents refrain from getting their kids vaccinated, but now with a cancer context.
Belief That Childhood Illnesses Are Not All That Dangerous
For many of these diseases, parents wrongly believe that they’re innocuous, a mere inconvenience in their lives. No big deal. They’ve bought into the erroneous idea that vaccines may do more harm than the disease ever could. They’ve never seen children hospitalized and/or dying from measles, diphtheria, or whooping cough (pertussis) infections. Every one of these diseases can be fatal, but few parents personally know anyone who died from them. They think it won’t happen to their kids, or their friend’s kids. Out of sight, out of mind.
HPV-induced cancers are a significantly more serious medical issue than the usual spectrum of childhood illnesses. Let me share what I’ve learned about one of the two most prevalent HPV cancers (and the one I was diagnosed with): oropharyngeal (oral) cancer. Unless it’s detected very early, patients are not even eligible for surgery. It’s straight to radiation and chemo, with their accompanying side effects. Nausea. Vomiting. Tiredness. Radiation burns. Difficulty swallowing. Loss of taste. Damaged salivary glands. And that’s if it hasn’t spread yet. The vaccine would prevent most of the cancer-causing infections with HPV, and could cut the number of oropharyngeal cancer cases in men by 70 percent. Cancer prevention is always preferable to cancer treatment.
When you daydream about your kids growing up, you likely picture graduations, weddings, and grandchildren, not their funerals. Maybe what parents need to see is an illustrative display of guts and gore, something reminiscent of the movies used to scare the crap out of teenagers in high school drivers ed classes. Imagine a series of cancer horror films in the same vein as Mechanized Death, Wheels of Tragedy, or Highway of Agony. These days, that would take the form of YouTube videos showing how HPV infections can lead to bulging tumors, feeding tubes, disfigured patients, and bereaved family members. Would this help turn the tide and up the vaccination rate?
Objection To Mandated Vaccination Requirements
Some parents resent being told by their state or local governments, or school districts, that they need to get their kids vaccinated against a variety of childhood diseases. For them, it’s an issue of freedom, being able to choose what’s right for their kids. That’s NOT the case with the HPV vaccine. Only three jurisdictions (RI and VA, along with the District of Columbia) currently mandate HPV vaccinations to attend school. Yes, many states have introduced legislation around HPV infections, but that simply funds vaccinations and/or educates families about the vaccine. Parents are simply being given the chance to make a good decision for their children. We need more of them to take advantage of this opportunity. These vaccines are truly lifesaving!
Interestingly, state mandates have not had an overall effect on HPV vaccine uptake, and the rates of vaccine initiation and completion were lower in mandated (vs. non-mandated) jurisdictions in the post-mandate period, and completion declined in mandated jurisdictions once mandates came into effect. See Polonijo, A.N. The impact of school-entry mandates on social inequalities in human papillomavirus vaccination. SSM - Population Health, Volume 12, December 2020, 100647 https://doi.org/10.1016/j.ssmph.2020.100647 FREE download. References in this article should also be looked at.
They Don’t Know About HPV Or The Cancers It Causes
Vaccinations against HPV differ from the ones given for most childhood diseases in three important ways: (1) the common childhood diseases are easily transmitted between kids via the air or casual contact. HPV cannot be passed that way. (2) HPV immunization is recommended for both boys and girls when they’re about 11 or 12, which is much later than for other childhood vaccines. (3) Unlike other childhood illnesses, where acute disease rapidly follows exposure, the cancer-causing effects of HPV only manifest themselves many years, or even decades, after infection.
Concerns That The Vaccine Will Lead Kids To Promiscuity
Because HPV is a sexually transmitted disease, some parents fear (as with birth control) that vaccination will quell their kids fears about sex. This will lead their children down the path to promiscuity. There’s simply no data that supports that conclusion. And while it’s clear that the virus is sexually transmitted, it’s unclear as to how that process takes place. Research on this subject is continuing.
Lack of Trust in Companies That Make Drugs in General, and Vaccines in Particular
People will say they simply don’t trust pharma companies to make vaccines that are both safe and effective. They argue that these companies are just in it for the money. Neither of these things are true. Pharma companies do have a bad reputation with the public due to a number of highly-publicized scandals over the past couple of decades. I wrote an opinion piece about this, Pharma’s tarnished reputation helps fuel the anti-vaccine movement, for those of who are interested in the subject.
Cost
Many parents think they can’t get their kids immunized against HPV because they simply don’t have the money to pay for it. They haven’t heard about the Vaccines for Children program of the CDC. It provides vaccines at no cost for children whose families have an inability to pay. The government buys the vaccines at a discount and sends them to providers who have signed up with the program. It’s not limited to the HPV vaccine and covers immunizations that will protect children from as many as 16 diseases. See the answer to the next question for more details about other ways to get the vaccine at no or reduced cost.
There are effective strategies for geting parents to vaccinate their kids against HPV. Here’s a link to a one hour video on Strategies for Recommending HPV Vaccination for Pre-teen Youth (2018) by Kristin Oliver, MD, MHS Icahn School of Medicine at Mt. Sinai.
The American Academy of Pediatrics also had suggestions for educating parents. Check out their HPV Champion Toolkit
You can also see recommendations from the American Cancer Society on this subject.
You can also check out this Powerpoint presentation on HPV infection and immunization rates in adolescents by Jennifer E. Dietrich, MD, Msc, Baylor College of Medicine. It looks at such issues as age of first intercourse (7% BEFORE the age of 13!), infection statistics of women, and vaccine coverage by different racial/ethnic groups.Does having had an HPV-caused cancer lead parents to vaccinate their kids against HPV more than other parents do? Using one’s own diagnosis to help decide on whether or not to treat a child is known as salience bias. You might think that women who had been diagnosed with HPV-caused cervical cancer, or pre-cancers, would be more inclined to vaccinate their kids against the virus. After all, they’ve experienced the most damaging effects of the virus. Despite this, a recent study showed that these women were no more likely to vaccinate their kids than women who had not had to deal with cervical cancer or pre-cancer treatment.
Why this is the case is unclear.
Worsham, C.M et al Association of Maternal Cervical Disease With Human Papillomavirus Vaccination Among Offspring. JAMA Netw Open. 2021;4(12):e2134566. doi:10.1001/jamanetworkopen.2021.34566 FREE download. -
34) Will Getting The HPV Vaccine Make Your Kids Promiscuous?
- There’s no need for parents to worry about this. First, a number of studies have shown that kids getting the vaccine don’t wind up having sex any more often than kids who don’t. Also, keep in mind that the vaccine, while protecting against HPV, does nothing to prevent other sexually transmitted infections, including gonorrhea, syphilis, chlamydia, herpes, and HIV. There are no vaccines to prevent these other sexually transmitted infections. Therefore, the HPV vaccine should really have little effect on whether or not kids have sex. Parents should remember that cancer prevention via the HPV vaccine beats having their kids someday need cancer treatment.
Here’s a recent cohort study you can look at that reinforces the message that the HPV vaccine does not lead to promiscuity: Brouwer, A.F. et al HPV vaccination has not increased sexual activity or accelerated sexual debut in a college-aged cohort of men and women. BMC Public Health201919:821. https://doi.org/10.1186/s12889-019-7134-1 FREE download.
You can also look at this paper published in the journal Pediatrics, Legislation to Increase Uptake of HPV Vaccination and Adolescent Sexual Behaviors. The authors concluded, “Implementation of HPV legislation was not associated with changes in adolescent sexual behaviors in the United States.”
Despite the fact that none of the world’s religions are opposed to vaccines, some religious schools in New Zealand are refusing to participate in government funded in-school vaccinations with the HPV vaccine. Most of these schools had a Christian religious background, and this ties into misinformation campaigns that the HPV vaccine somehow leads to teenage promiscuity. Study after study have debunked this myth.
Source: Some religious schools refusing to offer HPV vaccine. See FAQ 34 above for more details. -
35) Was A Story That The HPV Vaccine Caused Cervical Cancer Faked?
- This is a sad story and it’s true; a real example of “fake news”. This was apparently done as part of a deliberate effort to stop people from vaccinating their kids against HPV. The data was contained in an article in the Indian Journal of Medical Ethics entitled “Increased incidence of cervical cancer in Sweden: Possible link with HPV vaccination”. The paper was published under a pseudonym by someone claiming to be a member of the Karolinska Institute in Sweden. However, no one with that name ever worked there, and the paper was subsequently withdrawn from the journal. You can read more about the incident here. This also illustrates why one should be suspicious of articles published in obscure journals.
-
36) If HPV Infections Usually Clear Up On Their Own, Why Vaccinate?
- Because usually isn’t always. You don’t usually crash your car every time you drive it, but does that mean you don’t wear a seatbelt?
Your 5 year old doesn’t fall off her bike every time she rides it, but she still needs a helmet to keep her safe.
There is simply no way to predict today if your kids will be the lucky ones who are able to clear the infection, or if they’ll be unlucky ones who won’t. Let’s look at some of the numbers. It’s estimated that 14 million people in the US get infected with HPV every year. That’s a lot of people, and there are about 35,000 cases of HPV-caused cancer diagnosed each year. That includes all of the cancer sites: oropharyngeal and anal cancers in both genders, penile cancers in men, and vulval, vaginal, and cervical cancers in women (see FAQ6 on this page for details). And that’s just cancer. About 1% of people develop genital warts following HPV infection (see FAQ11 on this page), and the vaccine can prevent most of these as well. Finally, if you’re worried about rare side effects, keep in mind that more people are struck by lightning or attacked by a shark each year than suffer a serious adverse event from the vaccine (see FAQ 13 above). Vaccination is the smart choice for parents. -
37) How Many Countries Use The HPV Vaccine?
- According to the World Health Organization,
“116 Member States have introduced HPV vaccine by the end of 2021. Since many large countries have not yet introduced the vaccine and vaccine coverage decreased in 2021 in many countries, global coverage with the first dose of HPV among girls is now estimated at 15%. This is a proportionally large reduction from 20% in 2019.”
Note that the number of countries now vaccinating boys has increased in 2018 (see the question below).
The World Health Organization has recommended that ALL countries include the HPV vaccine in their routine vaccination schedules. However, if you look at the graphic below, you will see that there are many countries that have NOT yet introduced the vaccine as of 2019:
-
38) Do Some Countries Vaccinate Only Girls, But Not Boys?
- Yes. In fact, these countries are the rule, not the exception.
Since the launch of the World Health Organization's (WHO) global strategy to accelerate the elimination of cervical cancer in 2020, a further 30 countries, including Bangladesh, Indonesia, and Nigeria, have introduced a Human papillomavirus (HPV) vaccine into their vacation schedules.
As of November 17, 2023, 140 countries have now introduced HPV vaccinations into national programs.
Governments and communities are leading the way by declaring commitment and developing strategies to eliminate HPV cervical cancer, a sexually transmitted disease.
There are many countries that only vaccinate girls. I do not believe there are any countries that only vaccinate boys, not girls.
Let’s look at some other countries making news recently:
New countries adding the vaccine for girls:
Not all countries even have a policy of vaccinating girls, but this is slowly changing. On Oct. 10, 2018, Hong Kong officials announced that all school girls age 9-11 will be vaccinated against HPV. Vaccinations will be given at school. The goal is to decrease the number of cervical cancer cases. In 2015, there were 500 new cervical cancer cases in Hong Kong, and 169 women died of the disease. Taiwan also announced that they will start vaccinating girls at the end of 2018. Kenya announced it will provide the vaccine for free to girls starting in 2019 following a successful pilot program. Malawi will start vaccinating girls in 2019. Singapore will be providing free HPV vaccine to girls starting in 2019. Zimbabwe launched a campaign to vaccinate over a million girls in a week in May 2019. Costa Rica started vaccinating girls in June 2019. Kenya began vaccinating girls in Oct. 2019. Qatar will be adding HPV to their immunization schedules in 2020 (not clear the genders involved). Morocco started vaccinating girls in 2022, as did Sierra Leone. In 2023 Nigeria announced that it would be vaccinating 7.7 million girls age 9-14 against HPV. Thailand has plans to administer the HPV vaccine to female students nationwide, aged 11 to 20 years, starting in November 2023.
Another recent success story is the Philippines. While the government has a program for vaccinating girls, it does not reach those living in the poorer corners of the islands. Doctors Without Borders launched a massive vaccination program in the Tondo slums to vaccinate 25,000 girls between the ages of 9 and 13. Merck provided the vaccine at a discounted rate. You can read about this successful effort here.
Countries that have recently started to vaccinate boys:
Australia has been a leader in HPV vaccination. It mandated the HPV vaccine for girls beginning in 2007. In 2013, the mandate was expanded to boys. In 2017 New Zealand added boys in their HPV vaccination program as well.
The UK has just agreed to finally start vaccinating boys as part of the Department of Health and Social Care, although a start date for the vaccinations has not been announced. This will include England, Wales, and Scotland. Denmark announced in late 2018 that boys would get the HPV vaccine. Portugal announced that boys would get the HPV vaccine starting in 2019. Germany will start vaccinating boys in 2018 or 2019. Ireland will start vaccinating boys in 2019, as will Northern Ireland. Antigua will start vaccinating boys in 2019. I am trying to confirm that Belgium’s French-speaking Wallonia region and the Dutch speaking part of the country will start paying for HPV vaccines for boys as well! Guyana announced in 2019 that boys will get the HPV vaccine. The Netherlands are adding boys to the vaccination schedule in 2021. France is adding boys to the vaccination schedule starting in 2020. Finland will start immunizing boys in the fall of 2020.
Potential problem:
With so many countries in Europe coming on board to vaccinate boys, some at WHO have raised concerns that this will lead to a shortage of the vaccine for immunizing girls in poorer countries of the world. This issue may be ameliorated if dosing eventually switches from 2 or 3 doses per individual to a single dose. Several studies have now been done (see FAQ 1 above) indicating that a single dose of the vaccine may be equally active as the current multiple dose scheme. -
39) Are There Global Disparities In The Use Of The HPV Vaccine?
- Here’s an article from 2016 that looks at HPV vaccination rates globally. It explains why women in poor countries (where the vaccine is not generally available) remain at greater risk of developing cancer (especially cervical cancer) and dying from HPV than women from wealthier countries. See Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis: Bruni et al Lancet Vol. 4, No. 7, e453-3463 (2016).
One of the countries that has shown the greatest success in providing the HPV vaccine to girls is Rwanda, with 99% of school age girls vaccinated. To learn how they did this, take a look at How Rwanda could be the first country to wipe out cervical cancer. -
40) Are HPV Vaccines Mandated In Australia?
- Laws there are very strict indeed, and these apply to all required vaccines, not just the HPV vaccine. In 2016 the Australian federal government introduced a law called “no jab, no pay,” under which parents of unvaccinated children lose government benefits and welfare rebates — costing them up to 15,000 Australian dollars. That policy also didn’t allow for non-medical exemptions. You can get more details by reading this NY Times piece No Jab No Pay: How Australia is Handling Vaccinations.
There is legislation pending that would ban unvaccinated children in preschool and child care centers, and would fine these centers up to 30,000 Australian dollars, or about $24,000, if they allow an unvaccinated child to attend. Parents who object to vaccination on philosophical or religious grounds would not receive exemptions. The new laws are meant to combat the efforts of anti-vaccination groups.
As a result of their aggressive vaccination program for girls, Australia may become the first country to eradicate HPV-caused cervical cancers (according to the International Papillomavirus Society). You can read more about this in In Australia, Cervical Cancer Could Soon Be Eliminated, or look at this free paper in The Lancet The projected timeframe until cervical cancer elimination in Australia: a modelling study DOI:https://doi.org/10.1016/S2468-2667(18)30183-X
Compare this with the United States, where only three states have gotten rid of their personal belief exemptions that made it possible for parents to opt out of required vaccines because of their beliefs. California just did it in 2015, becoming only the third state — along with Mississippi and West Virginia — to have such a strict requirement. It’s much easier for parents in the other 47 states to opt out of having their children vaccinated for “personal reasons”, putting their kids and others at risk. -
41) Why Did Japan Stop Recommending The HPV Vaccine For Awhile?
- The HPV vaccine was introduced in Japan in 2013, and was widely accepted, and the percentage of girls being vaccinated in Japan was about 70 percent. The withdrawal of the vaccine recommendation several months after introduction happened because the government was concerned about adverse events associated with the vaccine. Note that government did NOT order the vaccine be taken off the market. They simply decided to stop recommending it. This was based on the fact that the Health Ministry was investigating 43 adverse events that were seen out of around 3.3 million HPV vaccinations given. This number was later bumped up to 176 adverse events, or 0.0019% of the cases. This is equal to about 1.9 events per 100,000 Gardasil vaccinations. The adverse events were temporally linked (that is, an event was noted after someone was immunized), but they could not establish a causal link to the vaccine. You can read more about this here.
In 2016, the Japan Expert Council on Promotion of Vaccination, representing seventeen Japanese academic health and medical societies involved in immunization, issued a statement appealing to the government to reverse the suspension and resume the proactive recommendation of the HPV vaccine based on the investigations and advice of the global scientific community. The government did nothing in response to this request, and this is where the situation still stands.
So did the vaccine work well in Japan while it was being given? We have a preliminary indication that this was indeed the case. I say preliminary because this info below was reported at a recent science meeting, and NOT in a published, peer reviewed journal. I will update this when the actual paper is published. Here is what the early data says, according to this Skeptical Raptor blog report:
“Results from a prospective cohort study of young Japanese women who received the HPV vaccine were presented to the Society of Gynecologic Oncology 50th Annual Meeting on Women’s Cancer which was held in Honolulu, Hawai’i in March 2019.
In this study, HPV screening and type-specific HPV testing were performed on 2,493 Pap test specimens collected from Japanese women aged 20 to 21 years during the period covering 2014 to 2017. Study participants provided HPV vaccination history through the completion of a questionnaire provided to the participants.
Here are some of the key results:
For the years 2014 to 2017, HPV vaccination rates were 28.6%, 74.8%, 76.7%, and 80.0%.
The prevalence of HPV 16/-18 infection (the subtypes most linked to cervical cancer) was 1.3% in 2014, 0.5% in 2015, 0.4% in 2016, and 0% in 2017. These are all statistically significant.
In 2014, the most prevalent strains were HPV-52, HPV-16, and HPV-56. HPV-52, HPV-51, and HPV-58 were most prevalent in 2017.
This study makes some very important observations. First, the Japanese HPV vaccine uptake has increased despite the Health Ministry error – it seems higher than the uptake in the USA which has never withdrawn recommendations for the vaccine.
Second, HPV 16/18 has apparently disappeared (or it’s so rare that it can’t be detected). This is powerful evidence for the effectiveness of the vaccine.
Finally, the population of HPV strains has shifted to HPV-52, HPV-51, and HPV-58. Of course, the “newer” Gardasil 9 protects against 52 and 58, so that will probably begin to reduce those subtypes.”
If you want to learn more about the HPV vaccine in Japan, read A Hundred Thousand Wombs by Riko Muranaka for a personal look at how rumors about the safety of HPV vaccine in Japan caused vaccination rates to plunge from about 70% to 1%. The author, a doctor, medical writer, and lecturer at Kyoto University won a prestigious award (the John Maddox prize) for exposing that data supporting a claim made by Dr. Ikeda that the “HPV vaccine is dangerous” were false. Ironically, Dr. Muranaka was later found guilty of defaming the researcher and ordered to pay him damages. According to the journal Science, “Ikeda had presented preliminary results based on an experiment with one mouse as “scientifically proven.” Japan’s health ministry issued a statement saying Ikeda’s results “have not proven anything about whether the symptoms that occurred after HPV vaccination were caused by the HPV vaccine,” and blasting him for his “very regrettable” responsibility in “causing misunderstanding among citizens.” Normile, D. Science (2019) Japanese court rules against journalist in HPV vaccine defamation case doi:10.1126/science.aax4915
The story is also covered in Why Japan’s HPV vaccine rates dropped from 70% to near zero, and how one doctor is fighting back.
Similarly problematic was another paper published by a Japanese group claiming that the HPV vaccine could lead to neurological damage. This paper, Murine hypothalamic destruction with vascular cell apoptosis subsequent to combined administration of human papilloma virus vaccine and pertussis toxin, was later retracted by the journal that published it, Nature Scientific Reports. The reasons given for retracting the paper included “the experimental setup, the use of a dose proportionally far larger than what is normally given, the use of the toxin, and inconsistencies between the data presented and the descriptions of results, among other issues.”
As a result of Japans essentially stopping giving the HPV vaccine, it’s been estimated that, if a vaccination catch-up program is NOT put in place, then there will be an additional 24,600–27,300 cervical cancer cases and 5,000–5,700 deaths over the lifetime of cohorts born between 1994 and 2007, compared with if coverage had remained at around 70% since 2013.
Simms, K.T. et al Impact of HPV vaccine hesitancy on cervical cancer in Japan: a modeling study. Lancet Public Health 2020. Published Online February 10, 2020 https://doi.org/10.1016/ S2468-2667(20)30010-4. FREE download.
In October 2021, a health ministry panel recommended that Japan actively resume promoting the use of human papillomavirus (HPV) vaccines, which would greatly boost the country’s low vaccination rate. In November of 2021, the health ministry announced that they would resume promoting the use of the vaccine in Japan. -
42) What's The WHO's Global Strategy For Eliminating Cervical Cancer?
- This strategy was announced on Nov. 17th, 2020. It outlines three key steps: vaccination, screening and treatment.
Successful implementation of all three could reduce more than 40% of new cases of the disease and 5 million related deaths by 2050.
This represents a historic milestone because it marks the first time that 194 countries commit to eliminating cancer following adoption of a resolution at this year’s World Health Assembly.
Meeting the following targets by 2030 will place all countries on the path toward elimination:
90% of girls fully vaccinated with the HPV vaccine by 15 years of age.
70% of women screened using a high-performance test by age 35 and again by 45.
90% of women identified with cervical disease receive treatment (90% of women with pre-cancer treated and 90% of women with invasive cancer managed).
The strategy also stresses that investing in the interventions to meet these targets can generate substantial economic and societal returns. An estimated US$ 3.20 will be returned to the economy for every dollar invested through 2050 and beyond, owing to increases in women’s workforce participation. The figure rises to US$ 26.00 when the benefits of women’s improved health on families, communities and societies are considered.
Cervical cancer is a preventable disease. It is also curable if detected early and adequately treated. Yet it is the fourth most common cancer among women globally. Without taking additional action, the annual number of new cases of cervical cancer is expected to increase from 570,000 to 700,000 between 2018 and 2030, while the annual number of deaths is projected to rise from 311,000 to 400,000. In low- and middle-income countries, its incidence is nearly twice as high and its death rates three times as high as those in high-income countries.
“The huge burden of mortality related to cervical cancer is a consequence of decades of neglect by the global health community. However, the script can be rewritten,” says WHO Assistant Director-General Dr Princess Nothemba (Nono) Simelela. “Critical developments include the availability of prophylactic vaccines; low-cost approaches to screening and treating cervical cancer precursors; and novel approaches to surgical training. Through a shared global commitment to the Sustainable Development Goals and leaving no-one behind, the countries of the world are forging a new path to ending cervical cancer. “
——————————————————————————————————————————————————————————————————————
This project supersedes the HPV-FASTER concept, where the basic goal was to speed up the elimination of cervical cancer across the world. The concept, proposed in 2016 by Xavier Bosch and colleagues, is a generalized HPV vaccination campaign aimed at females aged from 9 up to 30–45 years, paired with at least one HPV-screening test at any age above 30 years, and triage/diagnostic assessments of women who screen HPV positive. You can read more about this in HPV-FASTER: broadening the scope for prevention of HPV-related cancer. This article is an abridged version of Nat Rev Clin Oncol 13:119–132. doi:10.1038/nrclinonc.2015.146
——————————————————————————————————————————————————————————————————————
Note: a study in 2022 suggested that HPV vaccination alongside surgery for cervical lesions may reduce risk of further disease. However, the data were not definitive, and further studies are needed to see if this is actually true. The researchers noted that these effects were unclear because of (1) the scarcity of data and (2) the moderate to high overall risk of bias of the available studies.
Role of human papillomavirus (HPV) vaccination on HPV infection and recurrence of HPV related disease after local surgical treatment: systematic review and meta-analysis doi: 10.1136/ bmj-2022-070135 -
43) Did A Global Russian Cyberattack Interfere With HPV Vaccine Production?
- This is a true story. Merck, the manufacturer of the Gardasil 9 HPV vaccine, came under Russian cyberattack in the summer of 2017. The attack was NOT focused on Merck; they were simply collateral damage and their computers were not the primary focus of the assault. The attack was actually launched against Ukraine. The NotPetya cyberattack crippled the company’s computers for weeks, and as a resulted it greatly inhibited the ability of the company to make this life-saving vaccine. According to this article about the attack, “Merck estimated initially in regulatory filings that the malware did $870 million in damages. Among other things, NotPetya so crippled Merck’s production facilities that it couldn’t meet demand that year for Gardasil 9, the leading vaccine against the human papillomavirus, or HPV, which can cause cervical cancer. Merck had to borrow 1.8 million doses—the entire U.S. emergency supply—from the Pediatric National Stockpile. It took Merck 18 months to replenish the cache, valued at $240 million. (The Centers for Disease Control and Prevention say the stockpile’s ability to deliver medicine wasn’t affected.)”

A binary choice: cancer prevention with the vaccine, or someday possible treatment without it.